

Review
doi: 10.1182/blood-2005-04-1717.
Epub 2005 Jul 28.
Diagnosis and management of paroxysmal nocturnal hemoglobinuria
Affiliations
- PMID: 16051736
- PMCID: PMC1895106
- DOI: 10.1182/blood-2005-04-1717
Item in Clipboard
Review
Diagnosis and management of paroxysmal nocturnal hemoglobinuria
Blood.
.
No abstract available
Figures
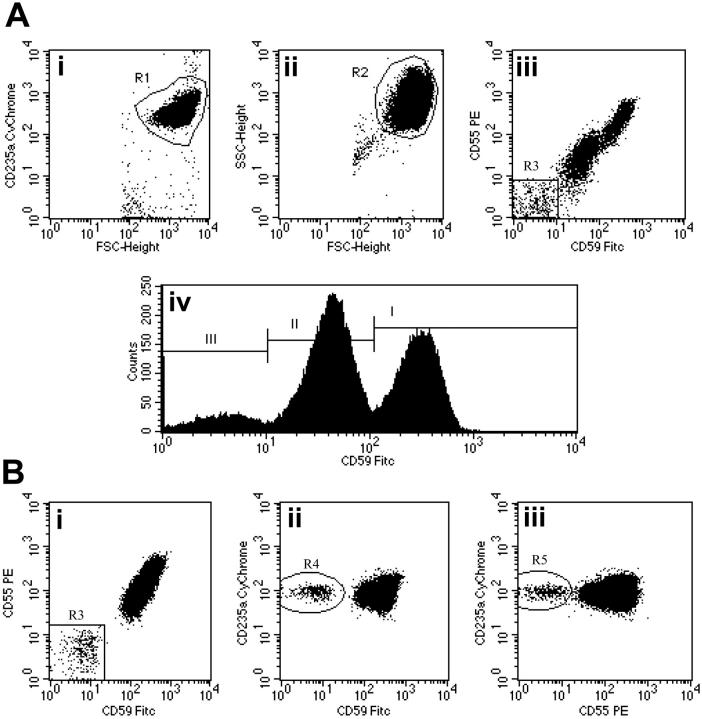
Flow cytometric analysis of red cells in PNH using a combination of anti-CD59 FITC, anti-CD55 PE, and anti-CD235a CyChrome. (Ai-ii) Flow cytometry plots show the gating strategy for identifying a pure population of red cells. An initial region (R1) is set on CD235a+FSCHigh events. A second region (R2) is then drawn around the logFSC/SSC characteristics of these cells. Only events that meet both these criteria are analyzed. (Aiii) CD59 and CD55 bivariate expression on these erythroid events. A small population of complete deficiency cells (type III) are detected (region R3 = 8.0%). (Aiv) Histogram analysis of CD59 expression also shows a major population of partially deficient cells (type II) comprising 53.9% of the total. Type I (normal expression) cells comprise 38.1% of the total. (Bi-iii) Detection of a very small red cell clone in a patient with PNH-sc/aplastic anemia. The red cell PNH clone comprises 0.4% of the total red cells (Bi). Confidence that this population is not an artifact is shown by simultaneous CD59 (Bii) and CD55 (Biii) deficiency and strong expression of CD235a. Illustration enhanced by A. Y. Chen.
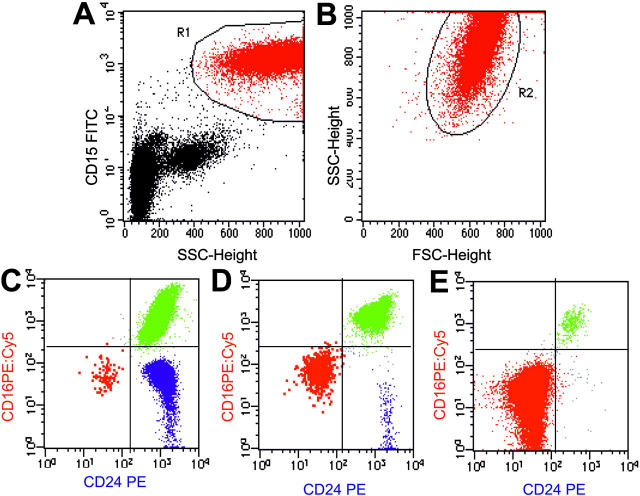
Flow cytometric analysis of granulocytes in PNH using a combination of anti-CD15 FITC, anti-CD24 PE, and anti-CD16 PE:Cy5. Flow cytometry plots (A-B) show the gating strategy for identifying a pure population of granulocytes based on light scatter characteristics and a transmembrane lineage marker (CD15). An initial region (R1) is set on CD15a+SSCHigh events (A). A second region (R2) is then drawn around the FSC/SSC characteristics of these cells to further refine the gating procedure (B). Only events that meet both these criteria are analyzed. (C-E) Using this combination, normal eosinophils (blue) can be clearly separated from PNH cells (red) and normal granulocytes (green). Plots are from 3 representative patients with PNH. (C) A small PNH granulocyte clone of 0.18% of total granulocytes in a patient with aplastic anemia (PNH-sc/aplastic anemia). (D) A larger PNH granulocyte clone of 8.7% in a patient with aplastic anemia (PNH/aplastic anemia). (E) Plot is from a patient with classic PNH and shows a large PNH granulocyte pool (98.8%). In this instance, the majority of hematopoiesis is derived from PNH stem cells. There is some residual normal granulocyte production (the 1% of cells that are CD16+CD24+) and this population serves as an internal positive control for antibody staining. Illustration enhanced by A. Y. Chen.
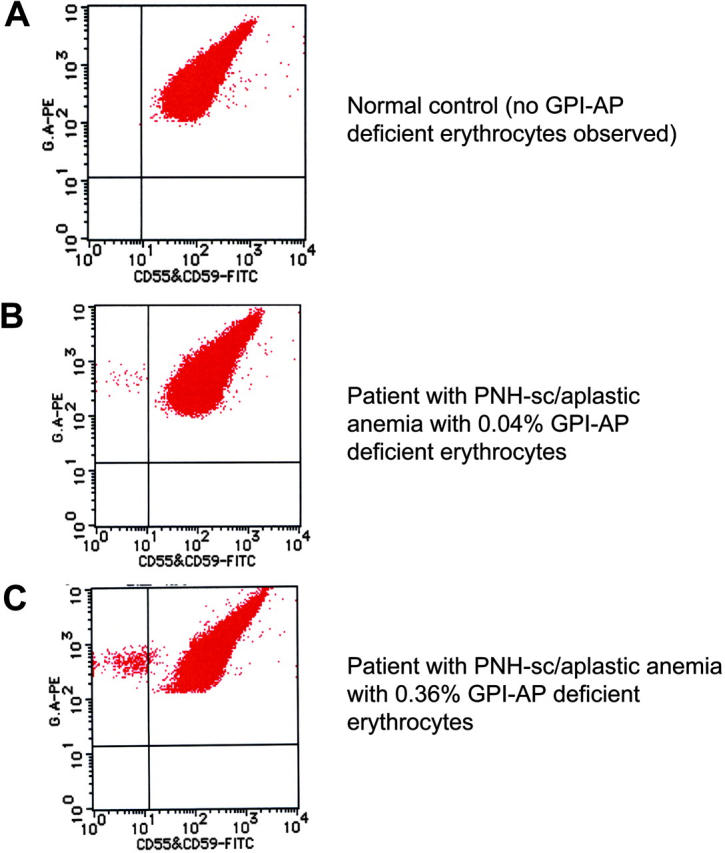
High-sensitivity flow cytometric analysis of erythrocytes. By careful gating and by using dual-color flow cytometry, GPI-deficient cells that comprise less than 1% of the total erythrocyte population can be reliably and reproducibly demonstrated (B-C). Using this technique, GPI-AP–deficient cells are not identified in the peripheral blood of the controls (volunteer donors; A). A combination of FITC-labeled anti-CD55 and anti-CD59 was used along with phycoerythrin (PE)–labeled anti–glycophorin A for the dual staining. These data were kindly provided by Dr Shinji Nakao and Dr Chiharu Sugimori, Kanazawa University, Japan, and are used with their permission. Illustration enhanced by A. Y. Chen.
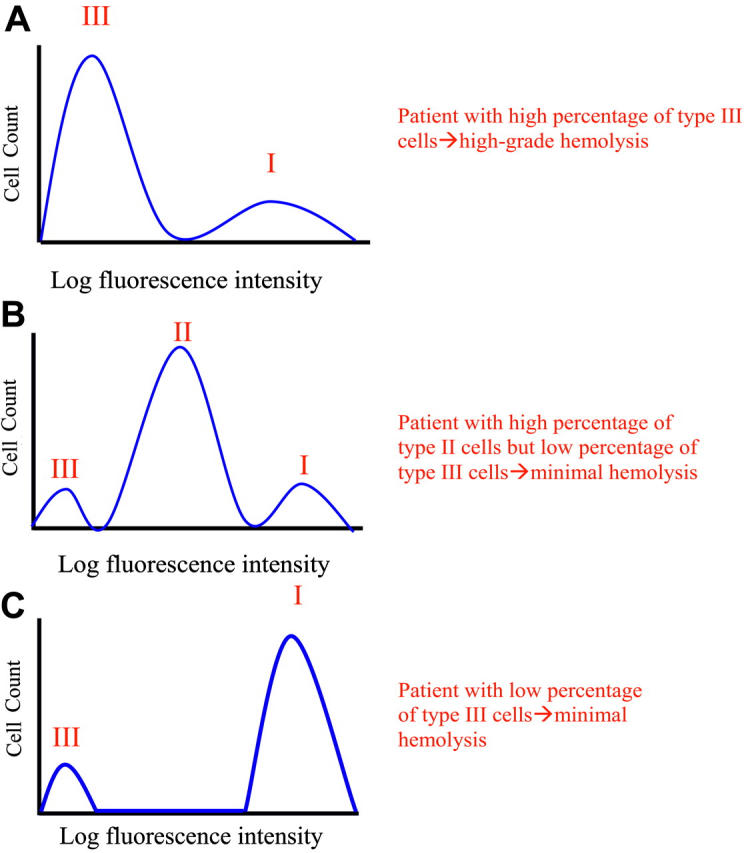
Phenotypic mosaicism in PNH. Hypothetical histograms of erythrocytes from patients with PNH stained with anti-CD59 are illustrated. The proportion and type of abnormal erythrocytes varies greatly among patients with PNH and these characteristics are important determinants of clinical manifestations. In general, patients with a high percentage of type III erythrocytes have clinically apparent hemolysis (A). If the erythrocytes are partially deficient in GPI-AP, hemolysis may be modest even if the percentage of the affected cells is high (B). A patient may have a diagnosis of PNH, but if the proportion of type III cells is low, only biochemical evidence of hemolysis may be observed (C). Illustration enhanced by A. Y. Chen.
References
-
- Dacie JV, Lewis SM. Paroxysmal nocturnal haemoglobinuria: clinical manifestations, haematology, and nature of the disease. Ser Haematol. 1972;5: 3-23. - PubMed
-
- Wang H, Chuhjo T, Yasue S, Omine M, Nakao S. Clinical significance of a minor population of paroxysmal nocturnal hemoglobinuria-type cells in bone marrow failure syndrome. Blood. 2002;100: 3897-3902. - PubMed
-
- Schubert J, Alvarado M, Uciechowski P, et al. Diagnosis of paroxysmal nocturnal haemoglobinuria using immunophenotyping of peripheral blood cells. Br J Haematol. 1991;79: 487-492. - PubMed
-
- Richards SJ, Rawstron AC, Hillmen P. Application of flow cytometry to the diagnosis of paroxysmal nocturnal hemoglobinuria. Cytometry. 2000;42: 223-233. - PubMed
-
- Hall SE, Rosse WF. The use of monoclonal antibodies and flow cytometry in the diagnosis of paroxysmal nocturnal hemoglobinuria. Blood. 1996; 87: 5332-5340. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
