

Toward a world consensus on prevention of schizophrenia
- PMID: 16060596
- PMCID: PMC3181724
- DOI: 10.31887/DCNS.2005.7.1/jvanos
Toward a world consensus on prevention of schizophrenia
Abstract
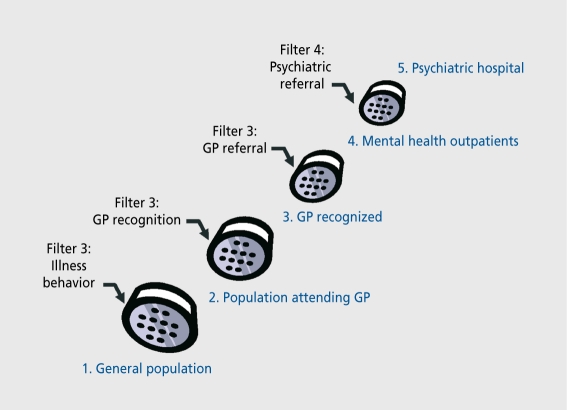
Screening for preschizophrenia in the general population with the aim of preventing transition to full-blown illness is an epidemiological impossibility because a rare disease cannot be predicted. The lack of specificity resulting in abundance of false-positives can be remedied in part by using much more restrictive screening criteria that combine several indicators of risk for transition to schizophrenia. Raising the specificity (reducing the false-positives), however, can only be done at the expense of sensitivity (increasing the false-negatives). The most commonly used strategy to raise specificity is the sample enrichment strategy. This involves the creation of samples enriched with schizophrenia risk by selectively filtering at-risk people out over a range of consecutive referral processes starting in the general population, through to general practioners, mental health services, and the early detection clinic. However, improvements in specificity obtained by the sample enrichment strategy should not be attributed to the use of some predictive instrument that supposedly identifies high-risk individuals. The epidemiologically and ethically most viable way for screening and early detection is to selectively increase the permeability of the filters on the pathway to mental health care. This will occasion samples of help-seekers enriched with schizophrenia risk at the level of mental health services (thus reducing false-positives), while at the same time making an attempt to "attract" as many detectable schizophrenia prodromes as possible through the filters along the pathway to mental health care (thus reducing false-negatives). Early psychosis research has yielded some useful suggestions in that it is becoming increasingly clear that it is not just psychosis itself, but rather the clinical context of the psychotic experience that determines risk for transition to schizophrenia. Thus, risk for transition to full-blown psychotic disorder is to a large degree determined by size of psychosis "load," comorbid distress and depression, cannabis use, cognitive ability, and subjective reports of impairment and coping. Making a diagnosis of psychotic disorder is not an exact science: it involves an arbitrary cutoff imposed on dimensional variation of psychopathology and need for care over time. Gaining insight into the cognitive and biological factors that drive the dimensional variation, including therapeutic interventions, is arguably more useful than sterile dichotomous prediction models.
La selección de sujetos pre-esquizofrénicos en la población general con el objetivo de prevenir la transición hacia la enfermedad totalmente constituída constituye una imposibilidad epidemiológica dado que una enfermedad poco frecuente no se puede predecir. La falta de especificidad, que da origen a gran cantidad de falsos positivos, puede ser remediada en parte al utilizar criterios de selección mucho más restrictivos que combinen algunos indicadores de riesgo para la transición hacia la esquizofrenia. Sin embargo, el aumento de la especificidad (reducción de falsos positivos) sólo puede realizarse a expensas de la sensibilidad (aumento de falsos negativos). La estrategia más comúnmente utilizada para aumentar la especificidad es el enriquecimiento de la muestra. Esta implica la creación de muestras enriquecidas con pacientes con riesgo de esquizofrenia mediante la filtración selectiva de sujetos con riesgo a partir de una serie de procesos de derivación consecutiva que se inician en la población general, a través de médicos generales, servicios de salud mental y clínicas para la detección precoz. Sin embargo, un aumento en la especificidad obtenido mediante la estrategia de enriquecimiento de la muestra no debe ser atribuido al empleo de algún instrumento predictor que presuntamente identifique individuos con alto riesgo. La forma de selección y detección precoz epidemiológica y éticamente más viable, es el aumento selectivo de la permeabilidad de los filtros en el camino hacia la atención en salud mental. Esto generará muestras de buscadores de ayuda enriquecidas con pacientes con riesgo de esquizofrenia a nivel de los servicios de salud mental (reduciendo así los falsos positivos) y al mismo tiempo se intentará "atraer" en cuanto sea posible a pacientes con pródromos esquizofrénicos detectables mediante filtros a lo largo del camino hacia la atención en salud mental (reduciendo así los falsos negativos). La investigación en psicosis precoces ha entregado algunas sugerencias útiles que están siendo cada vez más claras en el sentido que no sólo la psicosis en sí misma, sino que el contexto clínico de la experiencia psicótica es el que determina el riesgo de la transición hacia la esquizofrenia. De este modo, el riesgo de transición hacia el trastorno psicótico totalmente constituído está determinado en gran medida por el peso de la “carga” psicótica, el distrés y la depresión comórbidos, el empleo de cannabis, la capacidad cognitiva y las expresiones subjetivas de deterioro y adaptación. La realización del diagnóstico de un trastorno psicótico no constituye una ciencia exacta, sino que implica la imposición de un límite arbitrario a las variaciones en las dimensiones psicopatológicas y la necesidad de evaluación a lo largo del tiempo. El progreso en la comprensión de los factores cognitivos y biológicos que llevan a la variación de las dimensiones, incluyendo las intervenciones terapéuticas, es discutiblemente más útil que los estériles modelos de predicción dicotómica
Le dépistage d'état préschizophrénique dans la population générale dans le but d'empêcher le passage à la forme déclarée de la maladie est une impossibilité épidémiologique, parce qu'une maladie rare ne peut être anticipée. Le manque de spécificité dû à l'abondance des faux positifs peut être compensé en partie par des critères de dépistage plus restrictifs associant plusieurs indicateurs de risque pour le passage à la schizophrénie. L'augmentation de la spécificité (réduction des faux positifs) ne peut néanmoins se faire qu'aux dépens de la sensibilité (augmentation des faux négatifs). La méthode la plus répandue pour augmenter la spécificité est d'enrichir l'échantillon. Cela implique la création d'échantillons dans lesquels le risque schizophrénique est augmenté en filtrant sélectivement les individus à risque par une série d'orientations successives à partir de la population générale en passant par les médecins généralistes, les services de santé mentale et les services de détection clinique précoce. Néanmoins, ces améliorations de spécificité obtenues par cette méthode ne devraient pas être attribuées à l'utilisation de quelques instruments prédictifs supposés identifier les patients à haut risque. La méthode de dépistage et de détection précoce qui a le plus de chances de réussir épidémiologiquement et éthiquement est d'augmenter sélectivement la perméabilité des filtres sur le parcours vers les soins de santé mentale. Ceci produira des échantillons de demandeurs d'aide enrichis en risque schizophrénique dans les services de santé mentale (réduisant donc les faux positifs) en essayant d'attirer en même temps à travers ces filtres autant de prodromes schizophréniques que possible (réduisant donc les faux négatifs). La recherche de psychose précoce est à l'origine de quelques propositions utiles qui montrent de plus en plus clairement que ce n'est pas juste la psychose elle-même, mais le contexte clinique d'un épisode psychotique qui détermine le risque de passage à la schizophrénie. Le risque de passage à un état psychotique déclaré est donc largement déterminé par le poids de la «charge» psychotique, par l'existence d'une dépression et d'une souffrance comorbides, d'un usage de cannabis, par les capacités cognitives et les sentiments subjectifs exprimés de détérioration et de stratégies d'adaptation. Diagnostiquer un trouble psychotique ne relève pas d'une science exacte : cela implique une limite arbitraire imposée aux variations dimensionnelles en psychopathologie et la nécessité de soins au cours du temps. On peut dire qu'avancer dans la compréhension des facteurs biologiques et cognitifs qui commandent la variation dimensionnelle, y compris les interventions thérapeutiques, est sans doute plus utile que tes modèles stériles dichotomiques de prédiction.
Figures
Similar articles
-
Prediction of psychosis in adolescents and young adults at high risk: results from the prospective European prediction of psychosis study.Arch Gen Psychiatry. 2010 Mar;67(3):241-51. doi: 10.1001/archgenpsychiatry.2009.206. Arch Gen Psychiatry. 2010. PMID: 20194824
-
Risk factors for psychosis in an ultra high-risk group: psychopathology and clinical features.Schizophr Res. 2004 Apr 1;67(2-3):131-42. doi: 10.1016/S0920-9964(03)00192-0. Schizophr Res. 2004. PMID: 14984872
-
[Prevention in schizophrenia].Therapie. 2008 May-Jun;63(3):251-5. doi: 10.2515/therapie:2008032. Epub 2008 Aug 23. Therapie. 2008. PMID: 18718215 Review. French.
-
The prevention of schizophrenia.Int Rev Psychiatry. 2007 Dec;19(6):633-46. doi: 10.1080/09540260701797803. Int Rev Psychiatry. 2007. PMID: 18092241 Review.
-
Prediction of psychosis. A step towards indicated prevention of schizophrenia.Br J Psychiatry Suppl. 1998;172(33):14-20. Br J Psychiatry Suppl. 1998. PMID: 9764121
Cited by
-
Prodromal research: Public health initiatives for prevention of schizophrenia.Indian J Psychiatry. 2010 Jan;52(1):13-6. doi: 10.4103/0019-5545.58889. Indian J Psychiatry. 2010. PMID: 20174512 Free PMC article. No abstract available.
-
The Ohio State University Early Psychosis Intervention Center (EPICENTER) step-based care programme for individuals at clinical high risk for psychosis: study protocol for an observational study.BMJ Open. 2020 Jan 27;10(1):e034031. doi: 10.1136/bmjopen-2019-034031. BMJ Open. 2020. PMID: 31992606 Free PMC article.
-
Evidence that onset of clinical psychosis is an outcome of progressively more persistent subclinical psychotic experiences: an 8-year cohort study.Schizophr Bull. 2011 Jan;37(1):84-93. doi: 10.1093/schbul/sbp022. Epub 2009 May 21. Schizophr Bull. 2011. PMID: 19460881 Free PMC article.
-
A critique of the "ultra-high risk" and "transition" paradigm.World Psychiatry. 2017 Jun;16(2):200-206. doi: 10.1002/wps.20423. World Psychiatry. 2017. PMID: 28498576 Free PMC article.
-
Anticipating DSM-V: should psychosis risk become a diagnostic class?Schizophr Bull. 2009 Sep;35(5):841-3. doi: 10.1093/schbul/sbp071. Epub 2009 Jul 24. Schizophr Bull. 2009. PMID: 19633215 Free PMC article. No abstract available.
References
-
- Warner R. Early intervention in schizophrenia: a critique. Epidemiol Psichiatr Soc. 2002;11:248–255. - PubMed
-
- Cougnard A., Salmi LR., Verdoux H. A decade of debate on early intervention in psychosis: a systematic review of screening criteria. Schizophr Res. 2003;60:91–93. - PubMed
-
- Lencz T., Smith CW., Auther AM., Correll CU., Cornblatt BA. The assessment of “prodromal schizophrenia”: unresolved issues and future directions. Schizophr Bull. 2003;29:717–728. - PubMed
-
- Malla AM., Norman RM. Treating psychosis: is there more to early intervention than intervening early? Can J Psychiatry. 2001;46:645–648. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical