

Thyrotropin receptor-associated diseases: from adenomata to Graves disease
- PMID: 16075037
- PMCID: PMC1180562
- DOI: 10.1172/JCI26031
Thyrotropin receptor-associated diseases: from adenomata to Graves disease
Abstract
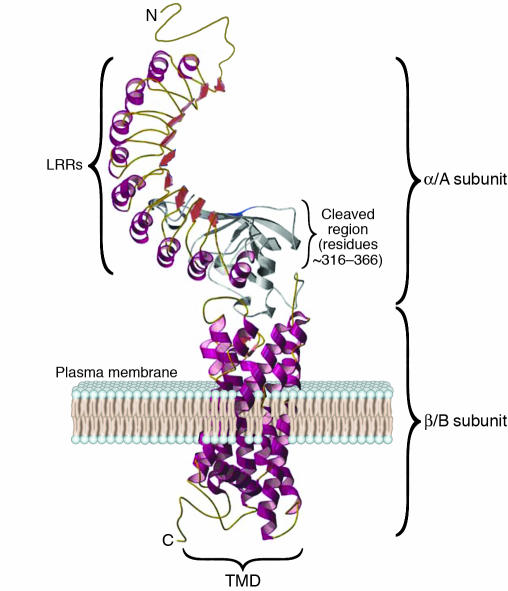
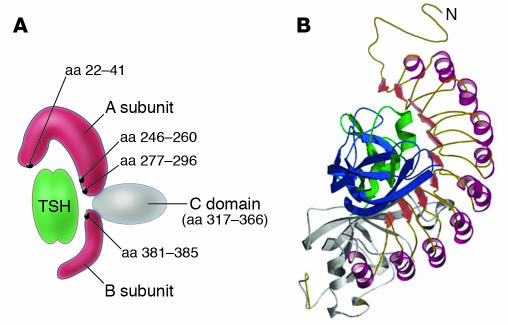
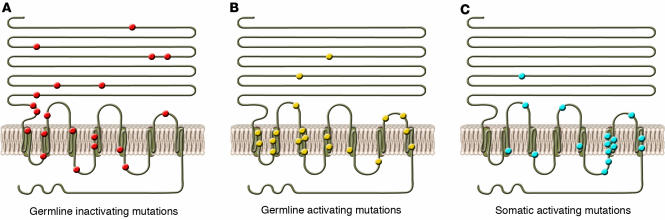
The thyroid-stimulating hormone receptor (TSHR) is a G protein-linked, 7-transmembrane domain (7-TMD) receptor that undergoes complex posttranslational processing unique to this glycoprotein receptor family. Due to its complex structure, TSHR appears to have unstable molecular integrity and a propensity toward over- or underactivity on the basis of point genetic mutations or antibody-induced structural changes. Hence, both germline and somatic mutations, commonly located in the transmembrane regions, may induce constitutive activation of the receptor, resulting in congenital hyperthyroidism or the development of actively secreting thyroid nodules. Similarly, mutations leading to structural alterations may induce constitutive inactivation and congenital hypothyroidism. The TSHR is also a primary antigen in autoimmune thyroid disease, and some TSHR antibodies may activate the receptor, while others inhibit its activation or have no influence on signal transduction at all, depending on how they influence the integrity of the structure. Clinical assays for such antibodies have improved significantly and are a useful addition to the investigative armamentarium. Furthermore, the relative instability of the receptor can result in shedding of the TSHR ectodomain, providing a source of antigen and activating the autoimmune response. However, it may also provide decoys for TSHR antibodies, thus influencing their biological action and clinical effects. This review discusses the role of the TSHR in the physiological and pathological stimulation of the thyroid.
Figures
References
-
- Duprez L, et al. Pathology of the TSH receptor. J. Pediatr. Endocrinol. Metab. 1999;12(Suppl. 1):295–302. - PubMed
-
- Rapoport B, Chazenbalk GD, Jaume JC, McLachlan SM. The thyrotropin (TSH) receptor: interaction with TSH and autoantibodies [review] Endocr. Rev. 1998;19:673–716. - PubMed
-
- Parmentier M, et al. Molecular cloning of the thyrotropin receptor. Science. 1989;246:1620–1622. - PubMed
