

Inherited disorders of voltage-gated sodium channels
- PMID: 16075039
- PMCID: PMC1180550
- DOI: 10.1172/JCI25505
Inherited disorders of voltage-gated sodium channels
Abstract
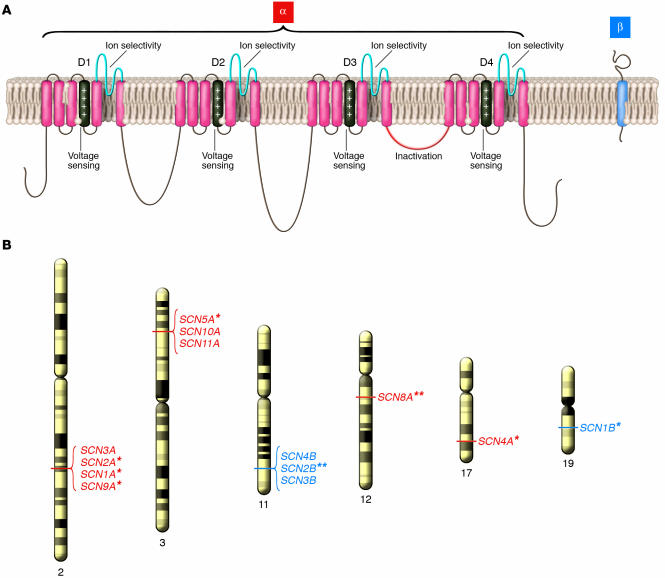
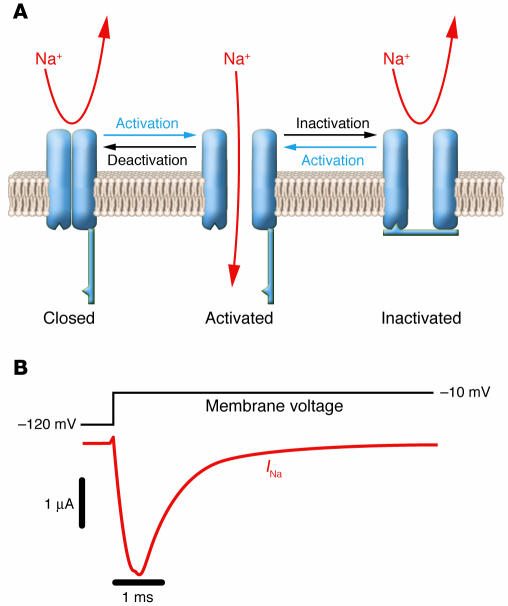
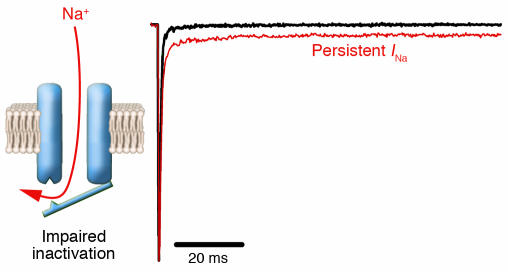
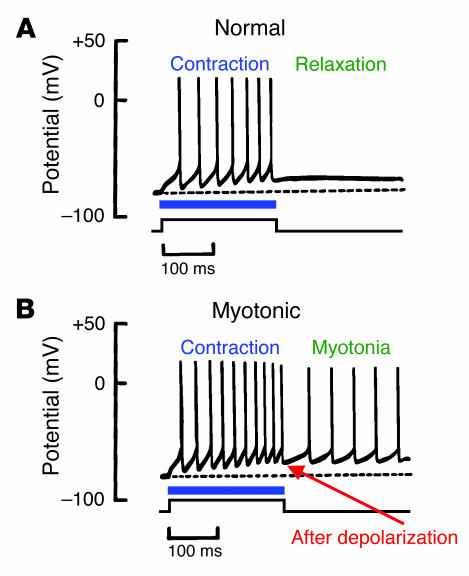
A variety of inherited human disorders affecting skeletal muscle contraction, heart rhythm, and nervous system function have been traced to mutations in genes encoding voltage-gated sodium channels. Clinical severity among these conditions ranges from mild or even latent disease to life-threatening or incapacitating conditions. The sodium channelopathies were among the first recognized ion channel diseases and continue to attract widespread clinical and scientific interest. An expanding knowledge base has substantially advanced our understanding of structure-function and genotype-phenotype relationships for voltage-gated sodium channels and provided new insights into the pathophysiological basis for common diseases such as cardiac arrhythmias and epilepsy.
Figures
References
-
- Catterall WA. Cellular and molecular biology of voltage-gated sodium channels [review] Physiol. Rev. 1992;72(Suppl. 4):S15–S48. - PubMed
-
- Catterall WA. From ionic currents to molecular mechanisms: the structure and function of voltage-gated sodium channels. Neuron. 2000;26:13–25. - PubMed
-
- Whitaker WR, et al. Distribution of voltage-gated sodium channel alpha-subunit and beta-subunit mRNAs in human hippocampal formation, cortex, and cerebellum. J. Comp. Neurol. 2000;422:123–139. - PubMed
-
- Trimmer JS, et al. Primary structure and functional expression of a mammalian skeletal muscle sodium channel. Neuron. 1989;3:33–49. - PubMed
-
- George AL, Komisarof J, Kallen RG, Barchi RL. Primary structure of the adult human skeletal muscle voltage-dependent sodium channel. Ann. Neurol. 1992;31:131–137. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
