

Optimization and validation of a multiplexed luminex assay to quantify antibodies to neutralizing epitopes on human papillomaviruses 6, 11, 16, and 18
- PMID: 16085914
- PMCID: PMC1182182
- DOI: 10.1128/CDLI.12.8.959-969.2005
Optimization and validation of a multiplexed luminex assay to quantify antibodies to neutralizing epitopes on human papillomaviruses 6, 11, 16, and 18
Abstract
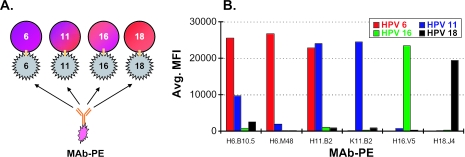
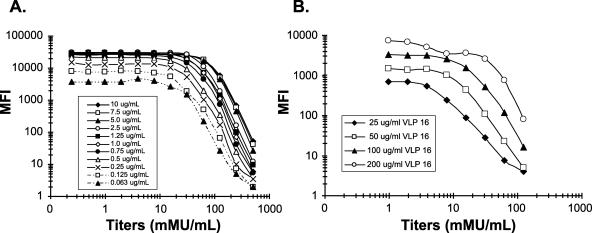
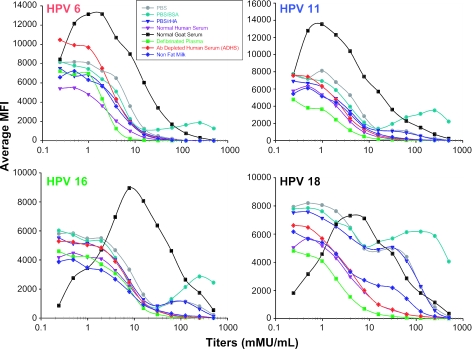
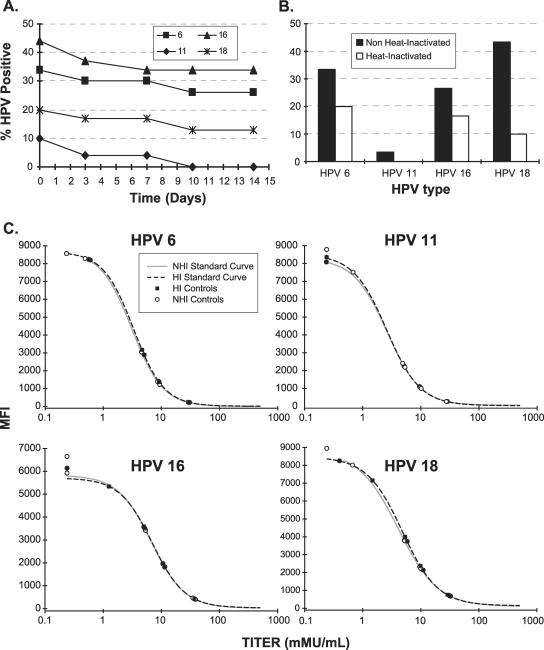
A human papillomavirus (HPV) multiplexed competitive Luminex immunoassay first described by Opalka et al. (D. Opalka, C. E. Lachman, S. A. MacMullen, K. U. Jansen, J. F. Smith, N. Chirmule, and M. T. Esser, Clin. Diagn. Lab. Immunol. 10:108--15, 2003) was optimized and validated for use in epidemiology studies and vaccine clinical trials. Optimization increased both the analytical sensitivity and the clinical specificity of the assay to more effectively discriminate the low-titer antibody response of HPV-infected persons from noninfected individuals. The characteristics of the assay that were optimized included monoclonal antibody (MAb) specificity, scaling up the conjugation of virus-like particles (VLPs) to microspheres, VLP concentration, MAb concentration, sample matrix, sample dilution, incubation time, heat inactivation of sample sera, and detergent effects on assay buffer. The assay was automated by use of a TECAN Genesis Workstation, thus improving assay throughput, reproducibility, and operator safety. Following optimization, the assay was validated using several distinct serum panels from individuals determined to be at low and high risk for HPV infection. The validated assay was then used to determine the clinical serostatus cutoff. This high-throughput assay has proven useful for performing epidemiology studies and evaluating the efficacy of prophylactic HPV vaccines.
Figures
References
-
- American Cancer Society. 2004. Cancer facts and figures 4. American Cancer Society, Atlanta, Ga.
-
- Atypical Squamous Cells of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesions Triage Study (ALTS) Group. 2000. Human papillomavirus testing for triage of women with cytologic evidence of low-grade squamous intraepithelial lesions: baseline data from a randomized trial. J. Natl. Cancer Inst. 92:397-402. - PubMed
-
- Bosch, F. X., M. M. Manos, N. Munoz, M. Sherman, A. M. Jansen, J. Peto, M. H. Schiffman, V. Moreno, R. Kurman, and K. V. Shah. 1995. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) study group. J. Natl. Cancer Inst. 87:796-802. - PubMed
-
- Carter, J. J., L. A. Koutsky, J. P. Hughes, S. K. Lee, J. Kuypers, N. Kiviat, and D. A. Galloway. 2000. Comparison of human papillomavirus types 16, 18, and 6 capsid antibody responses following incident infection. J. Infect. Dis. 181:1911-1919. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
