

Prospective analysis of clinical outcomes after percutaneous vertebroplasty for painful osteoporotic vertebral body fractures
- PMID: 16091504
- PMCID: PMC7975168
Prospective analysis of clinical outcomes after percutaneous vertebroplasty for painful osteoporotic vertebral body fractures
Abstract
Background and purpose: Previous studies have retrospectively reported the positive effects of percutaneous vertebroplasty. The purpose of our study was to evaluate prospectively the effects of vertebroplasty on mobility, analgesic use, pain, and SF-36 (short-form 36-item) scales for patients with painful vertebral compression fractures that are refractory to medical therapy.
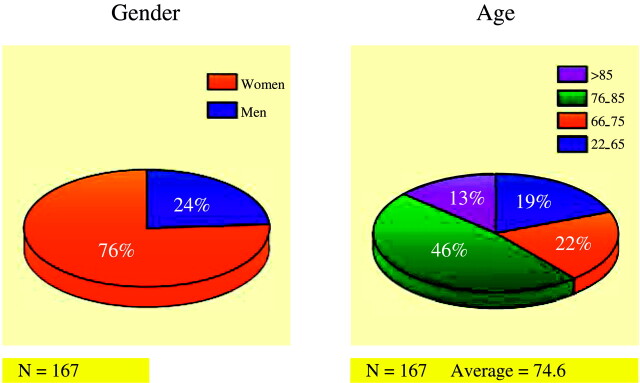
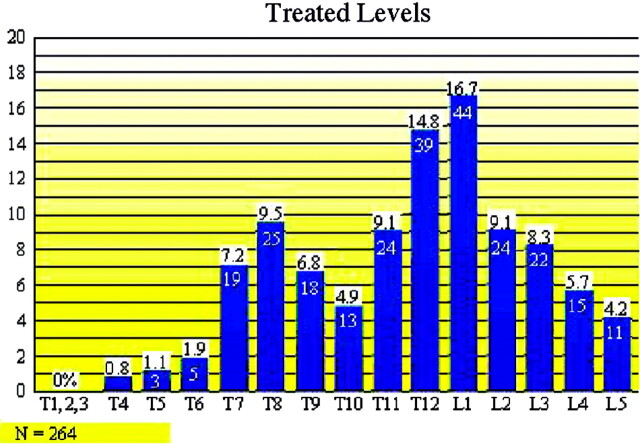
Methods: We prospectively followed 167 patients who received 207 vertebroplasty treatment sessions for stabilization of 264 symptomatic vertebral compression fractures between August 1999 and January 2003. The average age of patients was 74.6 years (SD = 12.2 years), and 76% were women. Pre- and postprocedural measurements of pain, mobility, analgesic use, and SF-36 scales were compared at 1 month after the procedure and between 6 months and 3 years after the procedure with the SF-36 scales.
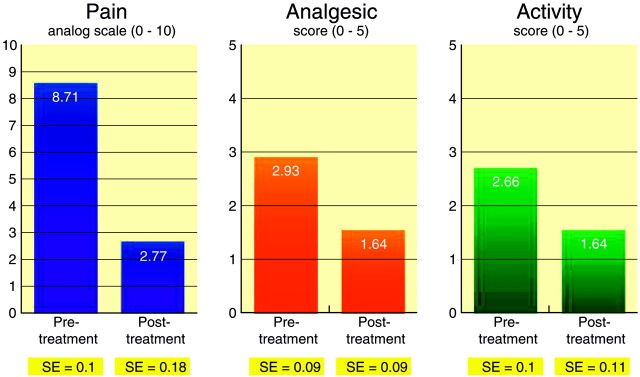
Results: Respective pre- and post-treatment pain scores were 8.71 (SE = 0.1) and 2.77 (SE = 0.18; P < .00001). Respective pre- and post-treatment analgesic use scores were 2.93 (SE = 0.9) and 1.64 (SE = 0.09; P < .00001). Respective pre- and post-treatment activity levels were 2.66 (SE = 0.1) and 1.64 (SE = 0.11; P < .00001). There was a statistically significant improvement on nine of 10 SF-36 scales (P < .001) after 1 month and on eight of 10 SF-36 scales (P < .02) at long-term follow-up.
Conclusion: Percutaneous vertebroplasty offers statistically significant benefits in decreasing pain, decreasing use of analgesics, and increasing mobility in appropriately selected patients. Percutaneous vertebroplasty also offers a statistically significant benefit in most SF-36 scales at both short- and long-term follow-up.
Figures

Comment in
-
Vertebroplasty and the randomized study: where science and ethics collide.AJNR Am J Neuroradiol. 2005 Aug;26(7):1610-1. AJNR Am J Neuroradiol. 2005. PMID: 16091502 Free PMC article. No abstract available.
References
-
- Riggs BL, Melton LJ III. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 1995;17:505S–511S - PubMed
-
- Melton LJ III. Epidemiology of spinal osteoporosis. Spine 1997;22(suppl 24):2S–11S - PubMed
-
- Jacobsen SJ, Cooper C, Gottlieb MS, et al. Hospitalization with vertebral fracture among the aged: a national population based study, 1986–1989. Epidemiology 1992;3:515–518 - PubMed
-
- Cotten A, Dewatre F, Cortet B, et al. Percutaneous vertebroplasty for osteolytic metastases and myeloma: effects of the percentage of lesion filling and the leakage of methyl methacrylate at clinical follow-up. Radiology 1996;200:525–530 - PubMed
-
- Deramond H, Depriester C, Galibert P, Le Gars D. Percutaneous vertebroplasty with polymethylmethacrylate. Radiol Clin North Am 1998;36:533–546 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical