

Spinal cord schistosomiasis: MR imaging appearance with surgical and pathologic correlation
- PMID: 16091508
- PMCID: PMC7975157
Spinal cord schistosomiasis: MR imaging appearance with surgical and pathologic correlation
Abstract
Background and purpose: Spinal cord involvement is a rare manifestation of schistosomiasis. We describe the MR imaging findings of spinal cord schistosomiasis in correlation with surgery and pathology.
Methods: We report eight cases of spinal cord schistosomiasis. All patients were men (mean age, 16.7 years) with neurologic manifestations who had been referred for spinal MR imaging. In all cases, spinal masses were surgically removed. MR imaging findings were correlated with surgery and pathology.
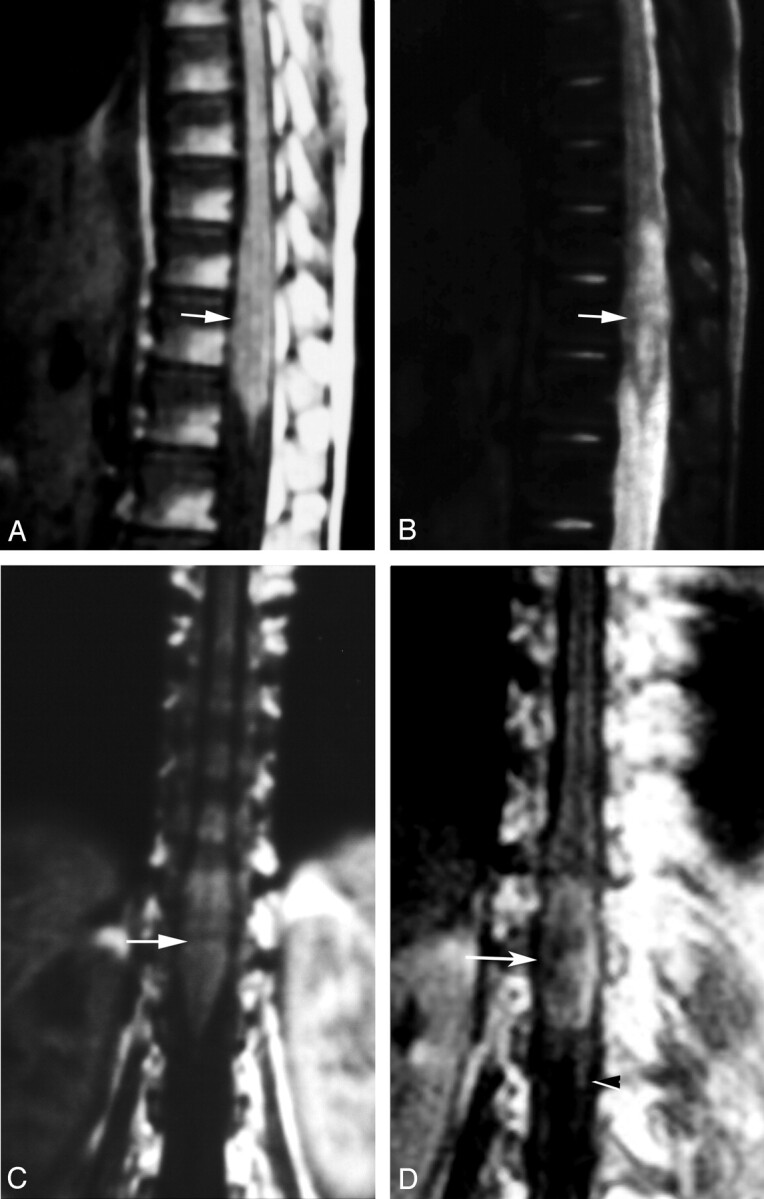
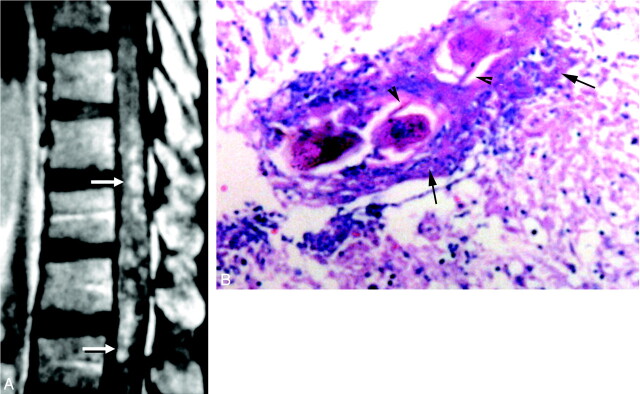
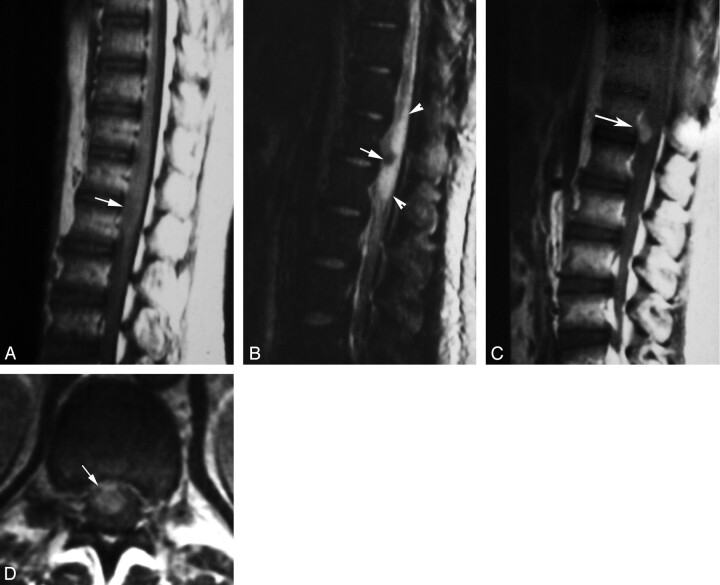
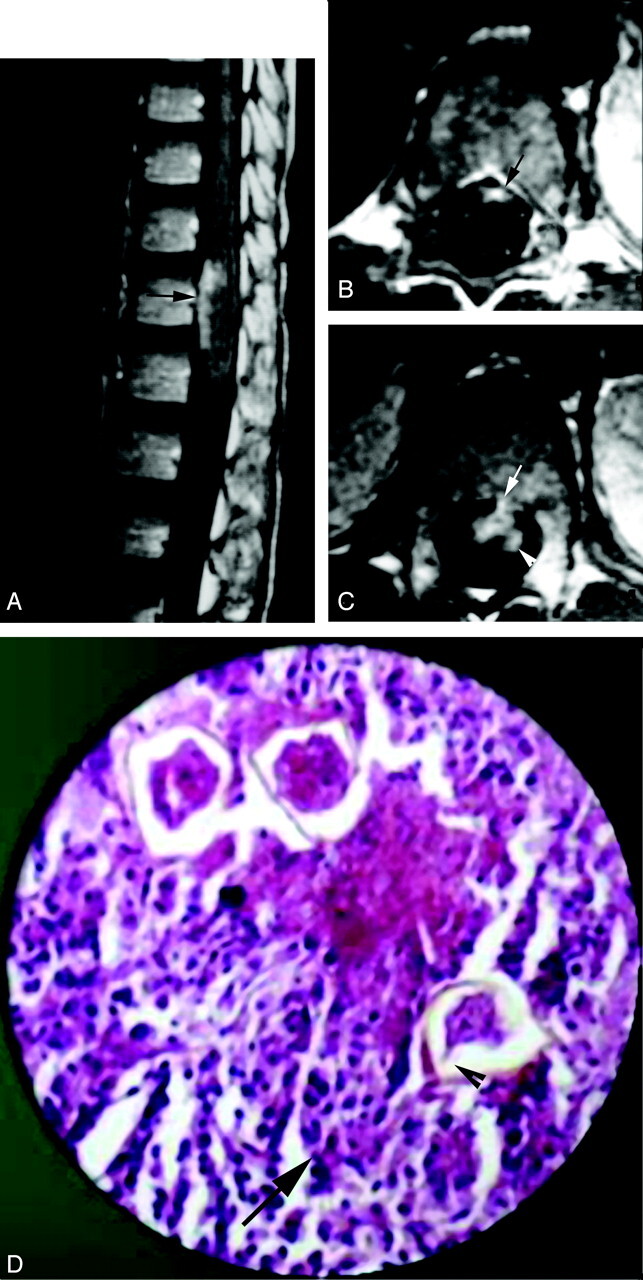
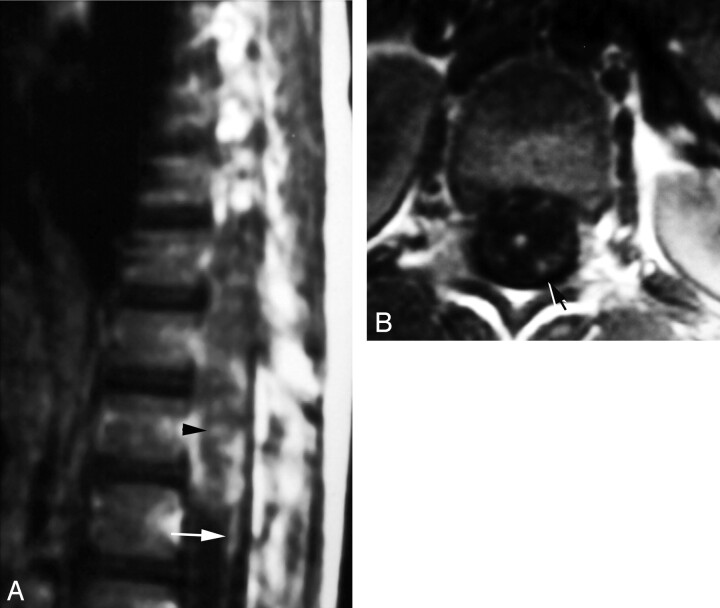
Results: MR imaging showed moderate expansion of the distal spinal cord in all cases. Abnormalities were isointense to cord in T1 and patchy hyperintense in T2-weighted spin-echo images (n = 8). Three forms of contrast enhancement were recognized: (1) intramedullary nodular (n = 8); (2) peripheral (n = 8); and (3) linear radicular (n = 4). Total gross surgical removal of masses by using the Cavitron ultrasonic surgical aspirator was possible in six cases. Diagnosis was established by identification of ova in histopathologic studies: Schistosoma mansoni (n = 3), S. hematobium (n = 1), and uncertain species (n = 4). Intramedullary nodular enhancement was correlated to multiple schistosomiasis microtubercles. Peripheral enhancing lesions correlated to thickened leptomeninges infested by chronic granulomatous inflammatory cells and schistosoma eggs. Linear radicular enhancement correlated with thickened resected nervous roots infested by granulomatous cells and schistosoma eggs.
Conclusion: Multinodular intramedullary contrast enhancement of the distal cord enabled correct presumptive preoperative MR imaging diagnosis of spinal schistosomiasis in three cases. Accurate diagnosis, through recognition of its MR imaging appearance, allows early treatment and better prognosis of spinal cord schistosomiasis.
Figures
References
-
- Mahmoud AA. Trematodes (schistosomiasis, other flukes). In: Mandell GL, Douglas RG, Bennet JE, eds. Principles and practice of infectious diseases. 2nd ed. New York: Wiley Medical;1985. :1573–1579
-
- El Banhawy A, Elwan O, Taher Y. Bilharzial granuloma of the conus medullaris and cuada equina. Paraplegia 1972;10:172–180 - PubMed
-
- Luyendijk W, Lindeman J. Schistosomiasis (Bilharziasis) mansoni of the spinal cord simulating an intramedullary tumor. Surg Neurol 1975;4:457–460 - PubMed
-
- Dar J, Zimmerman RR. Schistosomiasis of the spinal cord. Surg Neurol 1977;8:416–418 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical