

Disruption of cerebellar development: potential complication of extreme prematurity
- PMID: 16091510
- PMCID: PMC7975176
Disruption of cerebellar development: potential complication of extreme prematurity
Abstract
Background and purpose: Infants with very low birth weight are at high risk for cerebral lesions. Although supratentorial brain damage is a common radiologic finding, posterior fossa pathologies are rare. We studied the morphology of cerebellar involvement in a large series of 28 premature infants born before the 30th week of gestation to define typical patterns and identify possible risk factors for this pathology.
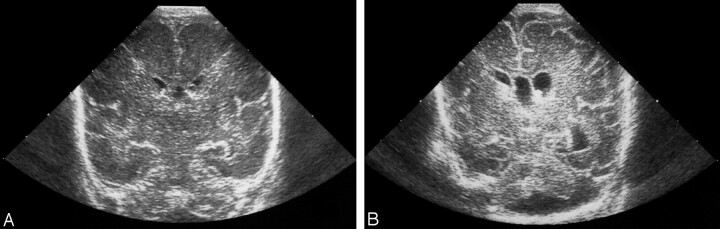
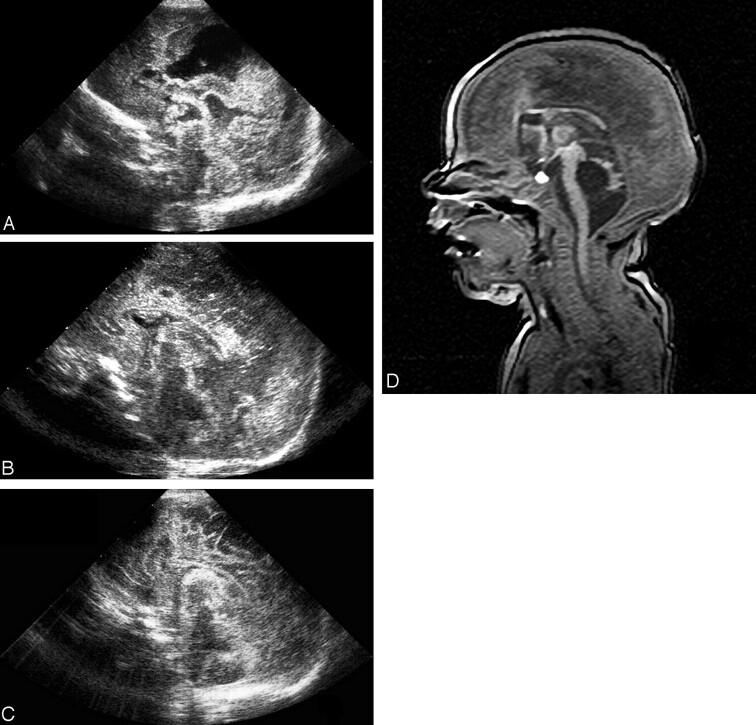
Methods: Cranial sonograms were obtained in the early neonatal period. MR imaging was performed between the 2nd month and the 6th year of life. Morphologic patterns of cerebellar involvement were evaluated.
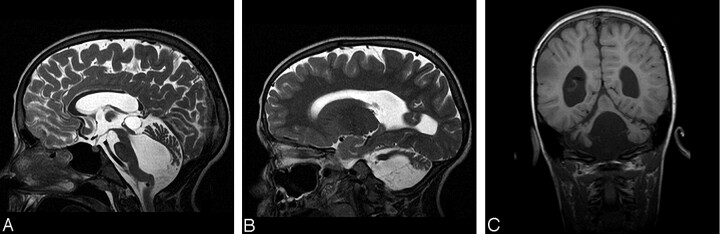
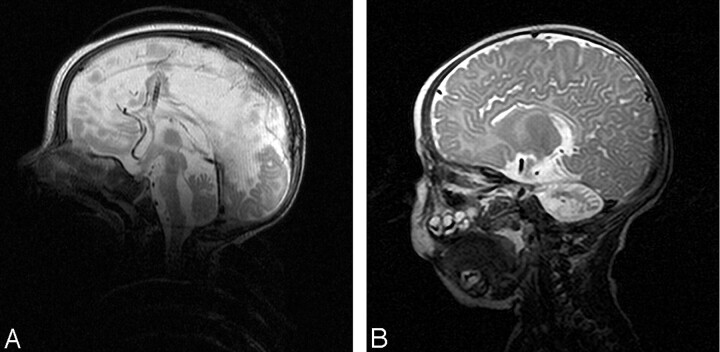
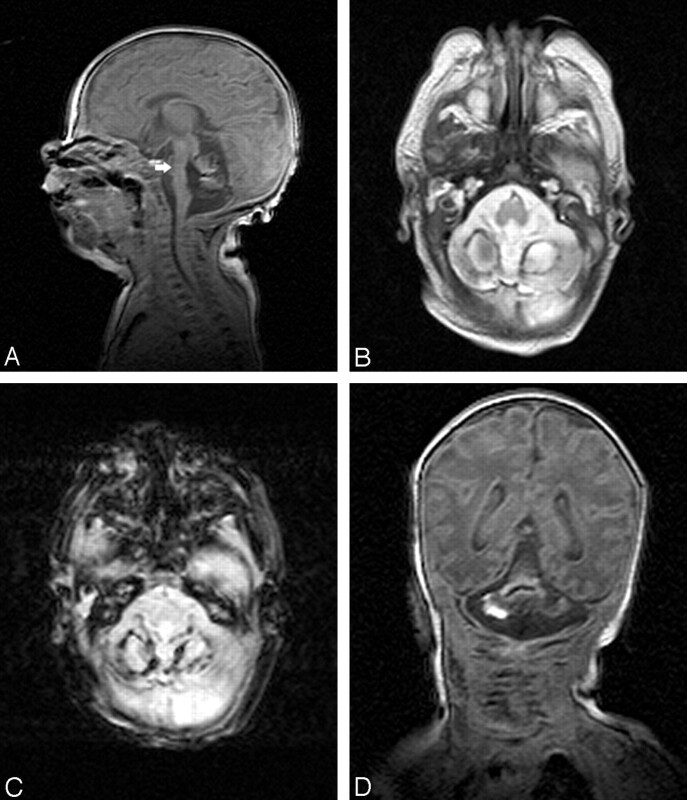
Results: Three morphologic patterns of cerebellar involvement were recognized: (1) symmetric volume reduction of the cerebellar hemispheres, which were floating immediately beneath the tentorium, and a small vermis with preserved shape; (2) symmetrical reduction in hemispheric volume with an enlarged, balloon-shaped fourth ventricle and a small, deformed vermis; and (3) normal overall cerebellar shape with extensive reduction of its dimensions. A small brain stem with flattened anterior curvature of the pons and loss of supratentorial white matter was present in all patients.
Conclusion: Symmetric cerebellar volume reduction was found as a consequence of extreme prematurity. Selective vulnerability of the developing cerebellum in the window of 24-30 weeks of gestation, combined with several additive perinatal risk factors (eg, hemosiderin deposits) seems to lead to destruction of immature structures and developmental arrest. Therefore, the resulting condition is the consequence of disrupted cerebellar development.
Figures

References
-
- Krägeloh-Mann I, Toft P, Lunding J, et al. Brain lesions in preterms: origin, consequences and compensation. Acta Paediatr 1999;88:897–908 - PubMed
-
- Rollins NK, Wen TS, Dominguez R. Crossed cerebellar atrophy in children: a neurologic sequela of extreme prematurity. Pediatr Radiol 1995;25 Suppl 1:S20–S25 - PubMed
-
- Mercuri E, He J, Curati WL, et al. Cerebellar infarction and atrophy in infants and children with a history of premature birth. Pediatr Radiol 1997;27:139–143 - PubMed
-
- Miall LS, Cornette LG, Tanner SF, et al. Posterior fossa abnormalities seen on magnetic resonance brain imaging in a cohort of newborn infants. J Perinatol 2003;23:396–403 - PubMed
-
- Merrill JD, Piechuch RE, Fell SC, et al. A new pattern of cerebellar hemorrhages in preterm infants. Pediatrics 1998;102:E62. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical