

Dural sinus compartment in dural arteriovenous shunts: a new angioarchitectural feature allowing superselective transvenous dural sinus occlusion treatment
- PMID: 16091520
- PMCID: PMC7975160
Dural sinus compartment in dural arteriovenous shunts: a new angioarchitectural feature allowing superselective transvenous dural sinus occlusion treatment
Abstract
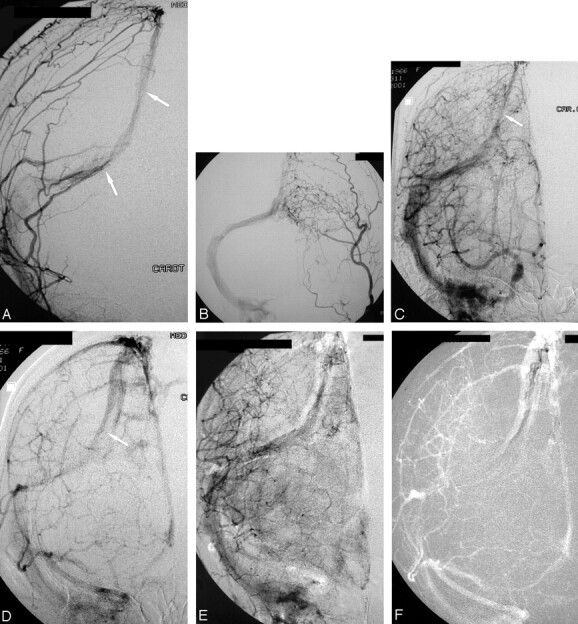
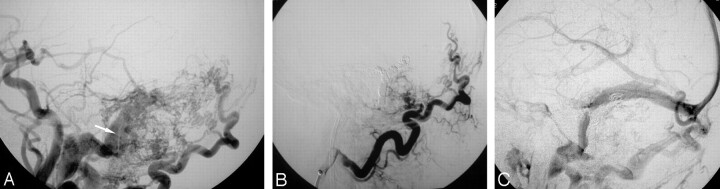
Background and purpose: The dural sinus occlusion has been shown to be effective in the treatment of some dural arteriovenous shunts (DAVS). No long-term results are available, however, regarding the significance of occlusion of a dural sinus. If the disease will stop or if other events will occur later in the remaining sinuses are not well known yet. Careful analyses of our cases led us to discover that, in some instances, the shunt involves only a single portion or compartment of a sinus. In this report, we describe our results in the treatment of these lesions: occluding only the involved compartment while preserving patency of the remainder of the sinus and the angiographic signals, thus allowing diagnosis of the presence of a compartment.
Methods and results: From 1996 to October 2002, we found 12 cases of DAVS (among 40 news cases of DAVS) with two types of compartments--one inside the sinus, which we call "septation" (nine cases), and the other outside the sinus, which we call "accessory sinus" (three cases). It was possible to occlude completely the lesion superselectively in nine cases. In two cases, it was necessary to occlude the entire sinus secondarily, and in one case the sinus was occluded because was impossible to catheterize the septation. Two cases with recanalization on the control were treated by additional arterial and arterial and venous approach.
Conclusion: It is very important to diagnose the presence of a compartment in dural arteriovenous shunts during the diagnostic angiography. In most cases, it allows curative treatment of the lesion by occluding only the compartment while preserving patency of the remainder of the sinus.
Figures




Similar articles
-
Transarterial intravenous coil embolization of dural arteriovenous fistula involving the superior sagittal sinus.Surg Neurol. 2001 Jun;55(6):353-8. doi: 10.1016/s0090-3019(01)00469-4. Surg Neurol. 2001. PMID: 11483194
-
Two unusual cases of multiple dural arteriovenous fistulas.Neurosurgery. 1997 Jul;41(1):288-92; discussion 292-3. doi: 10.1097/00006123-199707000-00051. Neurosurgery. 1997. PMID: 9218321
-
Transvenous embolization of dural fistulas involving the transverse and sigmoid sinuses.AJNR Am J Neuroradiol. 1989 Mar-Apr;10(2):385-92. AJNR Am J Neuroradiol. 1989. PMID: 2494858 Free PMC article.
-
Transvenous embolization for dural transverse sinus fistulas with occluded sigmoid sinus.Acta Neurochir (Wien). 2007;149(9):929-35; discussion 935-6. doi: 10.1007/s00701-007-1264-4. Epub 2007 Aug 13. Acta Neurochir (Wien). 2007. PMID: 17700989 Review.
-
[Dural arteriovenous fistula of the transverse sigmoid sinus after transvenous embolization of the carotid cavernous fistula].No To Shinkei. 1999 Dec;51(12):1065-9. No To Shinkei. 1999. PMID: 10654304 Review. Japanese.
Cited by
-
New Development of a Dural Arteriovenous Fistula (AVF) of the Superior Sagittal Sinus after Transvenous Embolization of a Left Sigmoid Sinus Dural AVF. Case Report and Review of the Literature.Interv Neuroradiol. 2006 Dec 15;12(4):363-8. doi: 10.1177/159101990601200412. Epub 2007 Jan 19. Interv Neuroradiol. 2006. PMID: 20569596 Free PMC article.
-
Toward a Better Understanding of Dural Arteriovenous Fistula Angioarchitecture: Superselective Transvenous Embolization of a Sigmoid Common Arterial Collector.AJNR Am J Neuroradiol. 2018 Sep;39(9):1682-1688. doi: 10.3174/ajnr.A5740. Epub 2018 Aug 16. AJNR Am J Neuroradiol. 2018. PMID: 30115674 Free PMC article.
-
Spontaneous Aggressive Conversion of Venous Drainage Pattern in Dural Arteriovenous Fistula Treated with Onyx Embolization.J Cerebrovasc Endovasc Neurosurg. 2016 Dec;18(4):396-401. doi: 10.7461/jcen.2016.18.4.396. Epub 2016 Dec 31. J Cerebrovasc Endovasc Neurosurg. 2016. PMID: 28184352 Free PMC article.
-
Turn-back embolization technique for effective transvenous embolization of dural arteriovenous fistulas.AJNR Am J Neuroradiol. 2012 Jun;33(6):E88-91. doi: 10.3174/ajnr.A2468. Epub 2011 May 5. AJNR Am J Neuroradiol. 2012. PMID: 21546461 Free PMC article.
-
Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes.Br J Radiol. 2012 Aug;85(1016):e395-403. doi: 10.1259/bjr/25192972. Epub 2012 Feb 28. Br J Radiol. 2012. PMID: 22374275 Free PMC article.
References
-
- Uflacker R, Lima SS, Ribas GC, Piske RL. Carotid-cavernour fistulas: embolization through the superior ophthalmic vein approach. Radiology 1986;159:175–179 - PubMed
-
- Deasy NP, Gholkar AR, Cox TCS, Jeffree MA. Tentorial dural arteriovenous fistulae: endovascular treatment with trans-venous coil embolization. Neuroradiology 1999;41:308–312 - PubMed
-
- Naito I, Iwai T, Shimaguchi H, et al. Percutaneous transvenous embolisation through the occluded sinus for transverse-sigmoid dural arteriovenous fistulas with sinus occlusion. Neuroradiology 2001;43:672–676 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous