

Endovascular treatment of posterior circulation cerebral aneurysms by using Guglielmi detachable coils: a 10-year single-center experience with special regard to technical development
- PMID: 16091522
- PMCID: PMC7975186
Endovascular treatment of posterior circulation cerebral aneurysms by using Guglielmi detachable coils: a 10-year single-center experience with special regard to technical development
Abstract
Background and purpose: The purpose of this study was to analyze the immediate and long-term angiographic and clinical results of endovascular treatment of posterior circulation aneurysms with special regard to technical development.
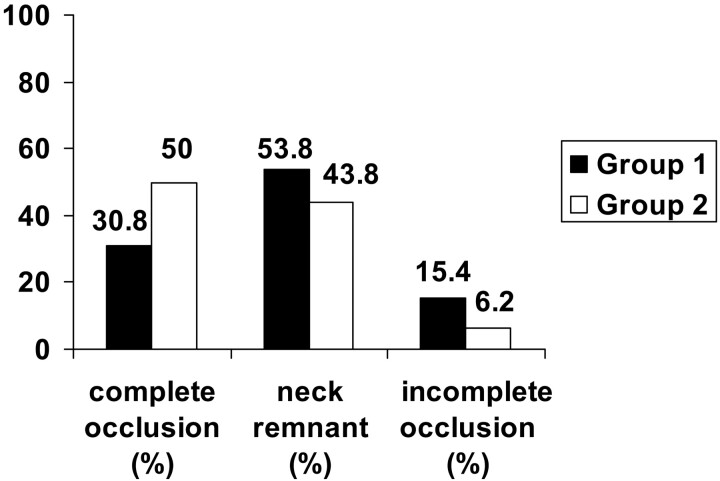
Materials: Between 1993 and 2003, 46 patients with 47 aneurysms of the posterior circulation were referred to our institution for endovascular treatment. Mean angiographic follow-up was 1.7 years. Clinical follow-up was determined at hospital discharge and by using a questionnaire for long-term follow-up (mean, 3.3 years). To analyze technical development, patients treated before (group 1) and after (group 2) implementation of 3D Guglielmi detachable coils (3D GDCs) in 1999 were compared. Multivariate analysis was performed to determine factors predictive of clinical and technical outcome.
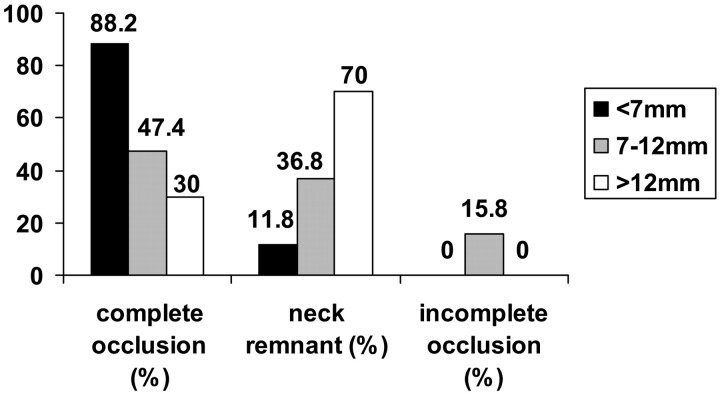
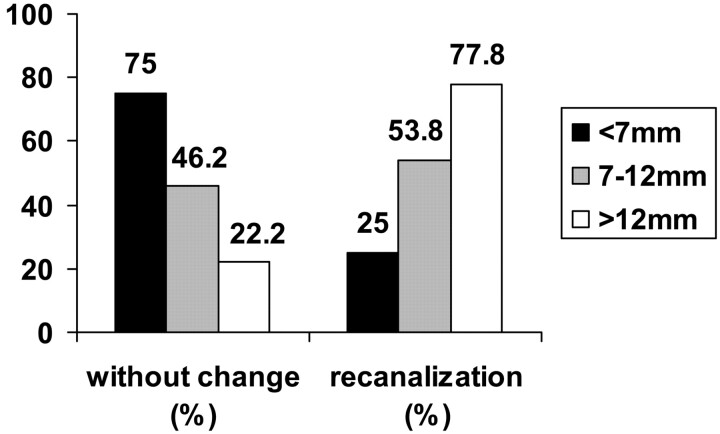
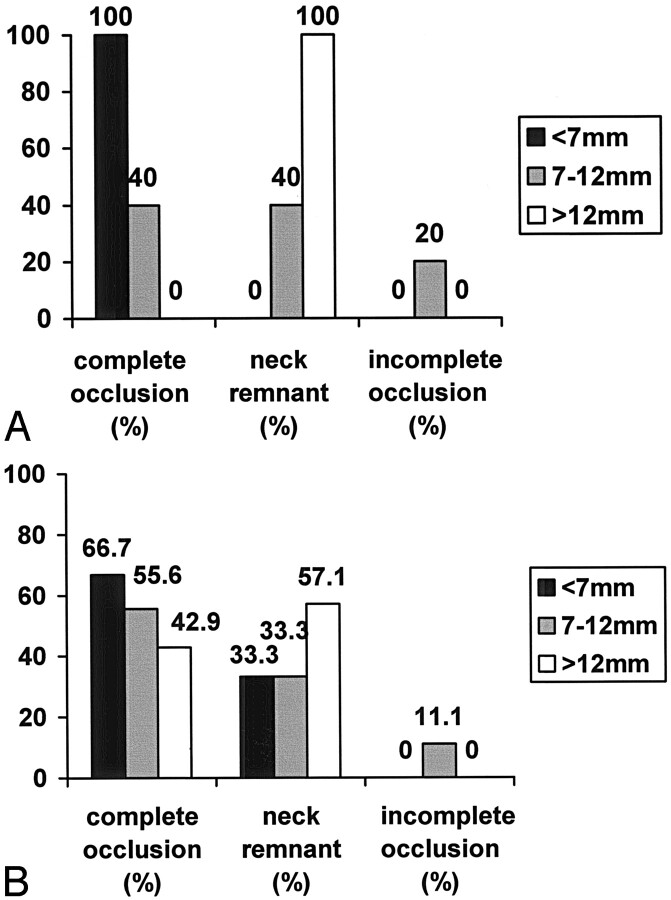
Results: Overall, at initial treatment complete occlusion was achieved in 27 (57.4%) aneurysms, a neck remnant was present in 16 (34.0%) aneurysms, incomplete occlusion was achieved in 3 (6.4%) aneurysms, and in 1 (2.1%) case occlusion was not attempted. Procedure-related permanent morbidity was 4.3%, and the mortality rate was 0%. There was no rebleeding of treated aneurysms. Complete occlusion at initial treatment (P = .003) and recanalization rate (P = .008) correlated with aneurysm sac size. A statistically significant relationship between Hunt and Hess/World Federation of Neurologic Surgeons clinical grading scale score and clinical outcome (Glasgow Outcome Score) was found (P < .05). Subgroup analysis revealed that a higher initial obliteration rate of larger aneurysms was achieved in group 2 (3D GDC, 22 patients, 22 aneurysms) than in group 1 (23 patients, 24 aneurysms; P = .03). At angiographic follow-up, overall recanalization was 47.1% in group 2 and 47.6% in group 1. Aneurysm neck size was not found to be correlated with occlusion and recanalization rate.
Conclusion: In our series, GDC technology was an effective and safe technique for the treatment of posterior circulation aneurysms. Aneurysm sac size was predictive for occlusion rate and the Hunt and Hess/World Federation of Neurologic Surgeons grade for clinical outcome. The introduction of 3D GDCs into our practice significantly improved the initial occlusion rate but did not affect the incidence of recanalization.
Figures
Similar articles
-
A multicenter study of 705 ruptured intracranial aneurysms treated with Guglielmi detachable coils.AJNR Am J Neuroradiol. 2005 Aug;26(7):1723-31. AJNR Am J Neuroradiol. 2005. PMID: 16091521 Free PMC article.
-
Endovascular treatment of basilar tip aneurysms with Guglielmi detachable coils: predictors of immediate and long-term results with multivariate analysis 6-year experience.Radiology. 2003 Mar;226(3):867-79. doi: 10.1148/radiol.2263011957. Epub 2003 Jan 24. Radiology. 2003. PMID: 12601216
-
Endovascular treatment of intracranial aneurysms with Guglielmi detachable coils: analysis of midterm angiographic and clinical outcomes.Stroke. 2002 Jan;33(1):210-7. doi: 10.1161/hs0102.100486. Stroke. 2002. PMID: 11779912
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Follow-up angiography of intracranial aneurysms treated with endovascular placement of Guglielmi detachable coils.Neurosurgery. 2002 Feb;50(2):239-49; discussion 249-50. doi: 10.1097/00006123-200202000-00003. Neurosurgery. 2002. PMID: 11844258 Review.
Cited by
-
Aneurysmal Subarachnoid Hemorrhage.J Neurosurg Anesthesiol. 2015 Jul;27(3):222-40. doi: 10.1097/ANA.0000000000000130. J Neurosurg Anesthesiol. 2015. PMID: 25272066 Free PMC article. Review.
-
Endovascular treatment of a vertebral artery aneurysm via puncture of the surgically exposed vertebral artery.Interv Neuroradiol. 2011 Mar;17(1):74-7. doi: 10.1177/159101991101700112. Epub 2011 Apr 29. Interv Neuroradiol. 2011. PMID: 21561562 Free PMC article.
-
Initial experience with an extremely soft bare platinum coil, ED coil-10 Extra Soft, for endovascular treatment of cerebral aneurysms.J Neurointerv Surg. 2013 Nov;5(6):577-81. doi: 10.1136/neurintsurg-2012-010498. Epub 2012 Nov 28. J Neurointerv Surg. 2013. PMID: 23190564 Free PMC article.
-
Multiple ruptured cerebral aneurysms at the National Hospital of the Kyrgyz Republic between 2008 and 2014: a departmental summary.Nagoya J Med Sci. 2019 Aug;81(3):511-518. doi: 10.18999/nagjms.81.3.511. Nagoya J Med Sci. 2019. PMID: 31579341 Free PMC article.
-
Modified buddy wire technique for coil embolization of posterior circulation aneurysms.Neuroradiology. 2007 Jan;49(1):49-55. doi: 10.1007/s00234-006-0154-4. Epub 2006 Nov 4. Neuroradiology. 2007. PMID: 17086408
References
-
- Malek AM, Higashida RT, Phatouros CC, et al. Treatment of an intracranial aneurysm using a new three-dimensional-shape Guglielmi detachable coil: technical case report. Neurosurgery 1999;44:1142–1145 - PubMed
-
- Guglielmi G, Vinuela F, Sepetka I, et al. Electrothrombosis of saccular aneurysms via endovascular approach. Part 1. Electrochemical basis, technique, and experimental results. J Neurosurg 1991;75:1–7 - PubMed
-
- Guglielmi G, Vinuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2. Preliminary clinical experience. J Neurosurg 1991;75:8–14 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical