

Health-related quality of life in patients with pulmonary arterial hypertension
- PMID: 16092961
- PMCID: PMC1208953
- DOI: 10.1186/1465-9921-6-92
Health-related quality of life in patients with pulmonary arterial hypertension
Abstract
Background: Improved outcomes with expanding treatment options for patients with pulmonary arterial hypertension present the opportunity to consider additional end-points in approaching therapy, including factors that influence health-related quality of life. However, comparatively little is known about health-related quality of life and its determinants in patients with pulmonary arterial hypertension.
Methods: Health-related quality of life was evaluated in a cross sectional study of 155 outpatients with pulmonary arterial hypertension using generic and respiratory-disease specific measurement tools. Most patients had either World Health Organization functional Class II or III symptoms. Demographic, hemodynamic and treatment variables were assessed for association with health-related quality of life scores.
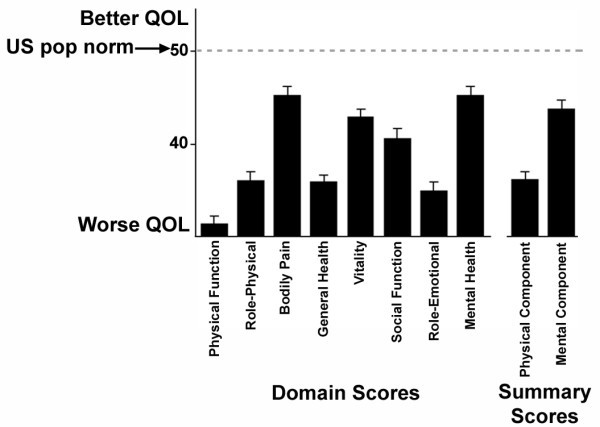
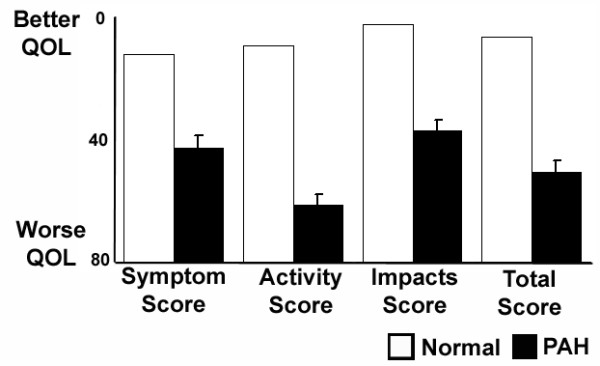
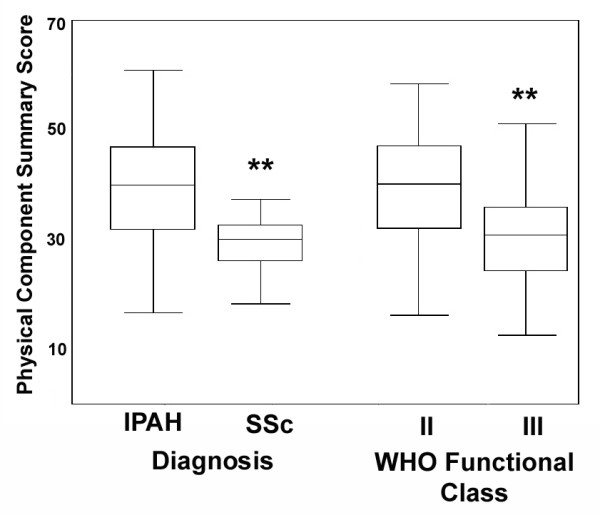
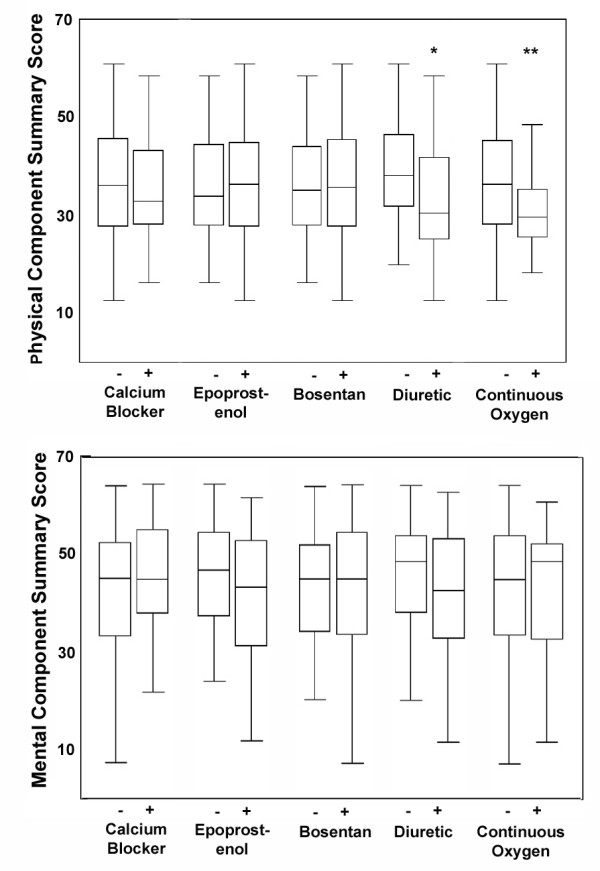
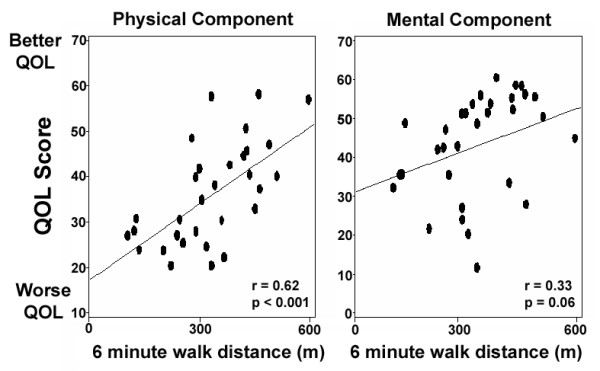
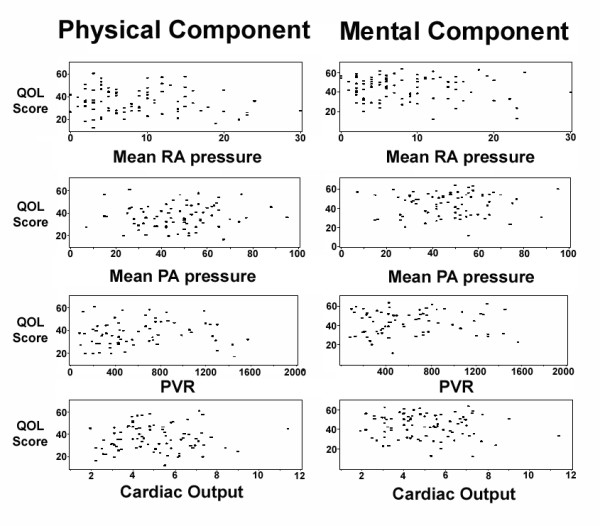
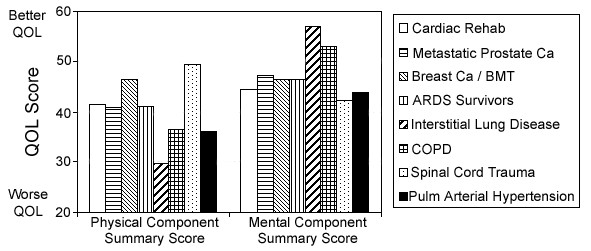
Results: Patients with pulmonary arterial hypertension suffered severe impairments in both physical and emotional domains of health-related quality of life. Patients with idiopathic ("primary") pulmonary arterial hypertension had the best, and those with systemic sclerosis the worst health-related quality of life. Greater six-minute walk distance correlated with better health-related quality of life scores, as did functional Class II versus Class III symptoms. Hemodynamic measurements, however, did not correlate with health-related quality of life scores. No differences in health-related quality of life were found between patients who were being treated with calcium channel antagonists, bosentan or continuously infused epoprostenol at the time of quality of life assessment.
Conclusion: Health-related quality of life is severely impaired in patients with pulmonary arterial hypertension and is associated with measures of functional status. Specific associations with impaired health-related quality of life suggest potential areas for targeted intervention.
Figures
References
-
- Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Koerner SK. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987;107:216–223. - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
