

Influence of continuous veno-venous hemofiltration on the course of acute pancreatitis
- PMID: 16097050
- PMCID: PMC4398728
- DOI: 10.3748/wjg.v11.i31.4815
Influence of continuous veno-venous hemofiltration on the course of acute pancreatitis
Abstract
Aim: To investigate whether continuous veno-venous hemofiltration (CVVH) in different filtration rate to eliminate cytokines would result in different efficiency in acute pancreatitis, whether the saturation time of filter membrane was related to different filtration rate, and whether the onset time of CVVH could influence the survival of acute pancreatitis.
Methods: Thirty-seven patients were classified into four groups randomly. Group 1 underwent low-volume CVVH within 48 h of the onset of abdominal pain (early CVVH, n = 9). Group 2 received low-volume CVVH after 96 h of the onset of abdominal pain (late CVVH, n = 10). Group 3 underwent high-volume CVVH within 48 h of the onset of abdominal pain (early CVVH, n = 9). Group 4 received high-volume CVVH after 96 h of the onset of abdominal pain (late CVVH, n = 9). CVVH was sustained for at least 72 h. Blood was taken before hemofiltration, and ultrafiltrate was collected at the start of CVVH and every 12 h during CVVH period for the purpose of measuring the concentrations of TNF-alpha, IL-1beta and IL-6. The concentrations of TNF-alpha, IL-1beta and IL-6 were measured by swine-specific ELISA. The Solartron 1 255 B frequency response analyzer (British) was used to observe the resistance of filter membrane.
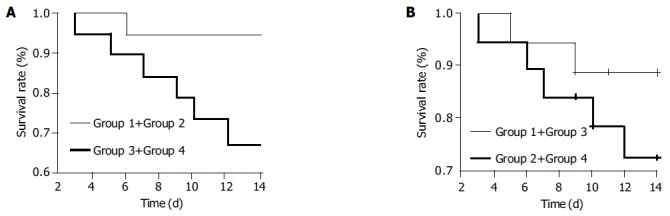
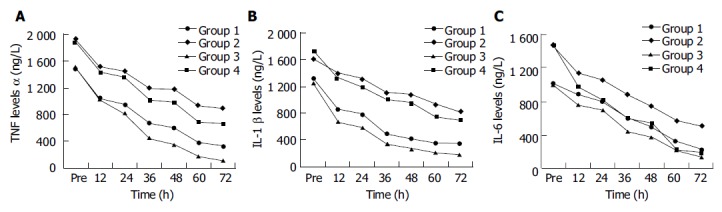
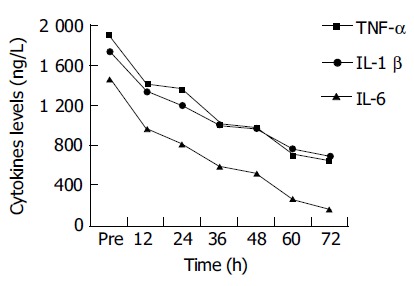
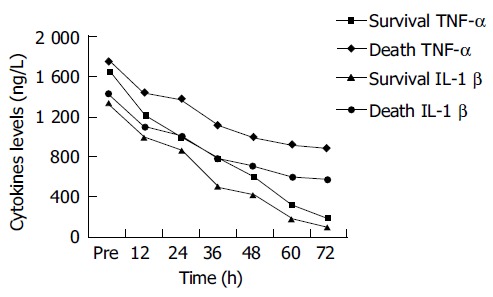
Results: The survival rate had a significant difference (94.44% vs 68.42%, P<0.01) high-volume and low-volume CVVH patients. The survival rate had also a significant difference (88.89% vs 73.68%, P<0.05) between early and late CVVH patients. The hemodynamic deterioration (MAP, HR, CVP) was less severe in groups 4 and 1 than that in group 2, and in group 3 than in group 4. The adsorptive saturation time of filters membranes was 120-180 min if the filtration rate was 1 000-4 000 mL/h. After the first, second and third new hemofilters were changed, serum TNF-alpha concentrations had a negative correlation with resistance (r: -0.91, -0.89, and -0.86, respectively in group 1; -0.89, -0.85, and -0.76, respectively in group 2; -0.88, -0.92, and -0.82, respectively in group 3; -0.84, -0.87, and -0.79, respectively in group 4). The decreasing extent of TNF-alpha, IL-1beta and IL-6 was significantly different between group 3 and group 1 (TNF-alpha P<0.05, IL-1beta P<0.05, IL-6 P<0.01), between group 4 and group 2 (TNF-alpha P<0.05, IL-1beta P<0.05, IL-6 P<0.01), between group 1 and group 2 (TNF-alpha P<0.05, IL-1beta P<0.05, IL-6 P<0.05), and between group 3 and group 4 (TNF-alpha P<0.01, IL-1beta P<0.01, IL-6 P<0.05), respectively during CVVH period. The decreasing extent of TNF-alpha and IL-1beta was also significantly different between survival patients and dead patients (TNF-alpha P<0.05, IL-1beta P<0.05). In survival patients, serum concentration of TNF-alpha and IL-1beta decreased more significantly than that in dead patients.
Conclusion: High-volume and early CVVH improve hemodynamic deterioration and survival in acute pancreatitis patients. High-volume CVVH can eliminate cytokines more efficiently than low-volume CVVH. The survival rate is related to the decrease extent of TNF-alpha and IL-1beta. The adsorptive saturation time of filter membranes are different under different filtration rate condition. The filter should be changed timely once filter membrane adsorption is saturated.
Figures
Similar articles
-
[Effects and mechanisms of high-volume hemofiltration on endotoxin-induced acute lung injury of piglets].Zhonghua Er Ke Za Zhi. 2017 May 4;55(5):343-348. doi: 10.3760/cma.j.issn.0578-1310.2017.05.007. Zhonghua Er Ke Za Zhi. 2017. PMID: 28482384 Chinese.
-
Cytokine removal and cardiovascular hemodynamics in septic patients with continuous venovenous hemofiltration.Intensive Care Med. 1997 Mar;23(3):288-96. doi: 10.1007/s001340050330. Intensive Care Med. 1997. PMID: 9083231 Clinical Trial.
-
Continuous veno venous hemofiltration in treatment of acute necrotizing pancreatitis.Chin Med J (Engl). 2003 Apr;116(4):549-53. Chin Med J (Engl). 2003. PMID: 12875720
-
Is continuous venovenous hemofiltration effective against severe acute pancreatitis?Artif Organs. 2013 Jul;37(7):615-22. doi: 10.1111/aor.12051. Epub 2013 Mar 5. Artif Organs. 2013. PMID: 23461644 Review.
-
Continuous veno-venous hemofiltration for severe acute pancreatitis.Cochrane Database Syst Rev. 2019 Oct 16;10(10):CD012959. doi: 10.1002/14651858.CD012959.pub2. Cochrane Database Syst Rev. 2019. PMID: 31618443 Free PMC article. Review.
Cited by
-
Effect of High-Volume Hemofiltration in Critically Ill Patients: A Systematic Review and Meta-Analysis.Med Sci Monit. 2019 May 28;25:3964-3975. doi: 10.12659/MSM.916767. Med Sci Monit. 2019. PMID: 31134957 Free PMC article.
-
Continuous veno-venous haemofiltration in the treatment of severe acute pancreatitis: 6-year experience.HPB (Oxford). 2007;9(4):295-301. doi: 10.1080/13651820701329225. HPB (Oxford). 2007. PMID: 18345308 Free PMC article.
-
Application of continuous renal replacement therapy (CRRT) in patients with severe acute pancreatitis: an analytical study.BMC Gastroenterol. 2025 Aug 18;25(1):592. doi: 10.1186/s12876-025-04198-y. BMC Gastroenterol. 2025. PMID: 40826030 Free PMC article.
-
Intensity of continuous renal replacement therapy for acute kidney injury.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD010613. doi: 10.1002/14651858.CD010613.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699760 Free PMC article.
-
Fluid resuscitation in acute pancreatitis.World J Gastroenterol. 2014 Dec 28;20(48):18092-103. doi: 10.3748/wjg.v20.i48.18092. World J Gastroenterol. 2014. PMID: 25561779 Free PMC article. Review.
References
-
- Gómez-Cambronero LG, Sabater L, Pereda J, Cassinello N, Camps B, Viña J, Sastre J. Role of cytokines and oxidative stress in the pathophysiology of acute pancreatitis: therapeutical implications. Curr Drug Targets Inflamm Allergy. 2002;1:393–403. - PubMed
-
- Tetta C, Bellomo R, Ronco C. Artificial organ treatment for multiple organ failure, acute renal failure, and sepsis: recent new trends. Artif Organs. 2003;27:202–213. - PubMed
-
- Schetz M. Non-renal indications for continuous renal replacement therapy. Kidney Int Suppl. 1999:S88–S94. - PubMed
-
- Oda S, Hirasawa H, Shiga H, Nakanishi K, Matsuda K, Nakamura M. Continuous hemofiltration/hemodiafiltration in critical care. Ther Apher. 2002;6:193–198. - PubMed
-
- Ronco C, Ricci Z, Bellomo R. Importance of increased ultrafiltration volume and impact on mortality: sepsis and cytokine story and the role for CVVH. Edtna Erca J. 2002;Suppl 2:13–18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
