

Neuropsychological characteristics of mild cognitive impairment subgroups
- PMID: 16103044
- PMCID: PMC2077558
- DOI: 10.1136/jnnp.2004.045567
Neuropsychological characteristics of mild cognitive impairment subgroups
Abstract
Objective: To describe the neuropsychological characteristics of mild cognitive impairment (MCI) subgroups identified in the Cardiovascular Health Study (CHS) cognition study.
Methods: MCI was classified as MCI-amnestic type (MCI-AT): patients with documented memory deficits but otherwise normal cognitive function; and MCI-multiple cognitive deficits type (MCI-MCDT): impairment of at least one cognitive domain (not including memory), or one abnormal test in at least two other domains, but who had not crossed the dementia threshold. The MCI subjects did not have systemic, neurological, or psychiatric disorders likely to affect cognition.
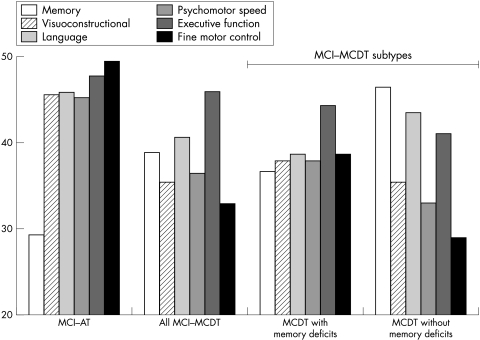
Results: MCI-AT (n = 10) had worse verbal and non-verbal memory performance than MCI-MCDT (n = 28) or normal controls (n = 374). By contrast, MCI-MCDT had worse language, psychomotor speed, fine motor control, and visuoconstructional function than MCI-AT or normal controls. MCI-MCDT subjects had memory deficits, though they were less pronounced than in MCI-AT. Of the MCI-MCDT cases, 22 (78.5%) had memory deficits, and 6 (21.5%) did not. MCI-MCDT with memory disorders had more language deficits than MCI-MCDT without memory disorders. By contrast, MCI-MCDT without memory deficits had more fine motor control deficits than MCI-MCDT with memory deficits.
Conclusions: The most frequent form of MCI was the MCI-MCDT with memory deficits. However, the identification of memory impaired MCI groups did not reflect the true prevalence of MCI in a population, as 16% of all MCI cases and 21.5% of the MCI-MCDT cases did not have memory impairment. Study of idiopathic amnestic and non-amnestic forms of MCI is essential for an understanding of the aetiology of MCI.
Conflict of interest statement
Competing interests: none declared
Similar articles
-
Executive functions deficit in mild cognitive impairment.Cogn Behav Neurol. 2007 Dec;20(4):219-24. doi: 10.1097/WNN.0b013e31815e6254. Cogn Behav Neurol. 2007. PMID: 18091070
-
[Classification of mild cognitive impairment in a population study].Rev Neurol. 2003 Jul 16-31;37(2):140-4. Rev Neurol. 2003. PMID: 12938073 Spanish.
-
Incidence of dementia in mild cognitive impairment in the cardiovascular health study cognition study.Arch Neurol. 2007 Mar;64(3):416-20. doi: 10.1001/archneur.64.3.416. Arch Neurol. 2007. PMID: 17353386
-
Mild cognitive impairment: a neuropsychological perspective.CNS Spectr. 2008 Jan;13(1):56-64. doi: 10.1017/s1092852900016163. CNS Spectr. 2008. PMID: 18204415 Review.
-
Language performance in Alzheimer's disease and mild cognitive impairment: a comparative review.J Clin Exp Neuropsychol. 2008 Jul;30(5):501-56. doi: 10.1080/13803390701550128. J Clin Exp Neuropsychol. 2008. PMID: 18569251 Review.
Cited by
-
Brain health correlates of mobility-related confidence.Exp Gerontol. 2022 Jun 15;163:111776. doi: 10.1016/j.exger.2022.111776. Epub 2022 Mar 24. Exp Gerontol. 2022. PMID: 35339632 Free PMC article.
-
Neuropsychological contributions to the early identification of Alzheimer's disease.Neuropsychol Rev. 2008 Mar;18(1):73-90. doi: 10.1007/s11065-008-9054-1. Epub 2008 Mar 18. Neuropsychol Rev. 2008. PMID: 18347989 Free PMC article. Review.
-
Identifying mild cognitive impairment at baseline in the Ginkgo Evaluation of Memory (GEM) study.Aging Ment Health. 2009 Mar;13(2):171-82. doi: 10.1080/13607860802380656. Aging Ment Health. 2009. PMID: 19347684 Free PMC article.
-
Improving the Methodology for Identifying Mild Cognitive Impairment in Intellectually High-Functioning Adults Using the NIH Toolbox Cognition Battery.Front Psychol. 2021 Sep 8;12:724888. doi: 10.3389/fpsyg.2021.724888. eCollection 2021. Front Psychol. 2021. PMID: 34566807 Free PMC article.
-
Longitudinal Patterns of Brain Changes in a Community Sample in Relation to Aging and Cognitive Status.J Alzheimers Dis. 2023;94(3):1035-1045. doi: 10.3233/JAD-230080. J Alzheimers Dis. 2023. PMID: 37355895 Free PMC article.