

Combined immunostimulation and conditional cytotoxic gene therapy provide long-term survival in a large glioma model
- PMID: 16103070
- PMCID: PMC1242178
- DOI: 10.1158/0008-5472.CAN-04-3434
Combined immunostimulation and conditional cytotoxic gene therapy provide long-term survival in a large glioma model
Abstract
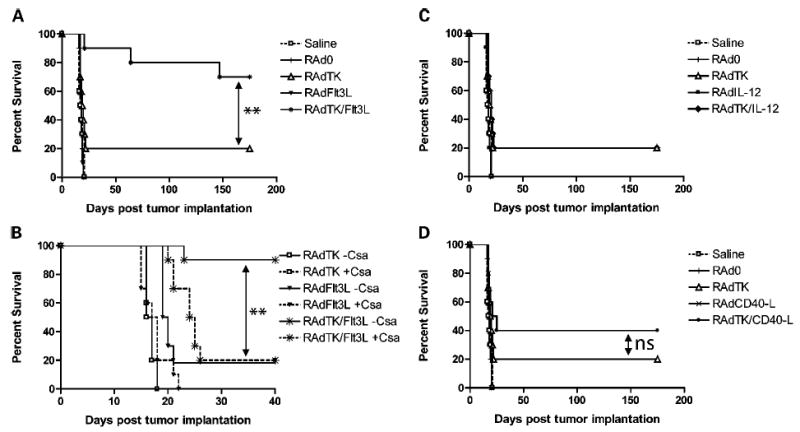
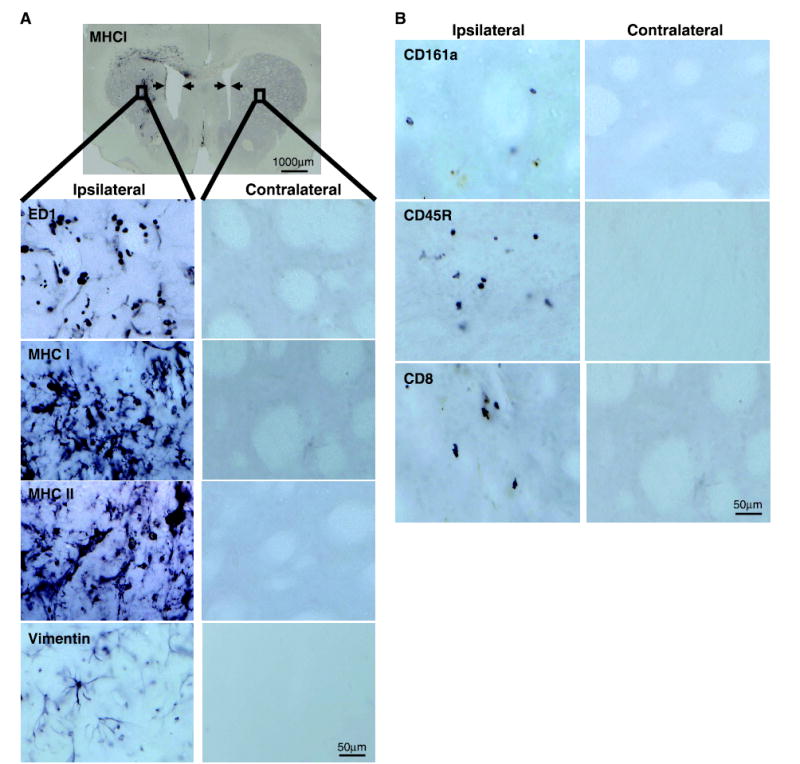
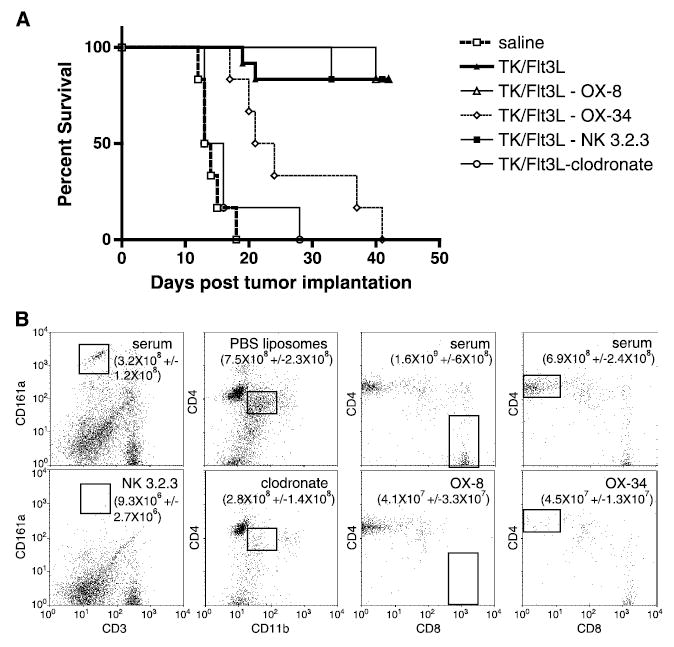
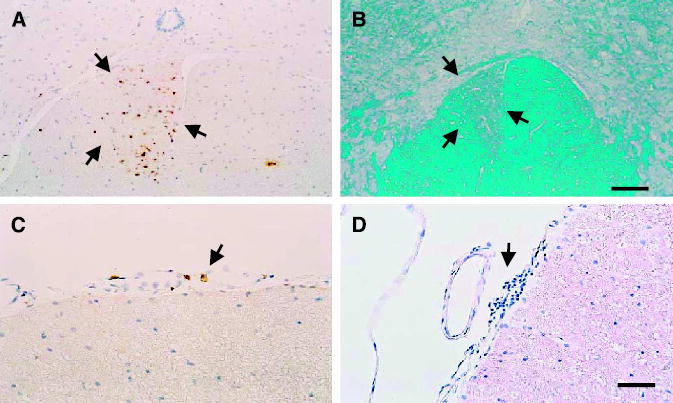
In spite of preclinical efficacy and recent randomized, controlled studies with adenoviral vectors expressing herpes simplex virus-1 thymidine kinase (HSV1-TK) showing statistically significant increases in survival, most clinical trials using single therapies have failed to provide major therapeutic breakthroughs. Because glioma is a disease with dismal prognosis and rapid progression, it is an attractive target for gene therapy. Preclinical models using microscopic brain tumor models (e.g., < or =0.3 mm3) may not reflect the pathophysiology and progression of large human tumors. To overcome some of these limitations, we developed a syngeneic large brain tumor model. In this model, administration of single therapeutic modalities, either conditional cytotoxicity or immunostimulation, fail. However, when various immunostimulatory therapies were delivered in combination with conditional cytotoxicity (HSV1-TK), only the combined delivery of fms-like tyrosine kinase ligand (Flt3L) and HSV1-TK significantly prolonged the survival of large tumor-bearing animals (> or =80%; P < or = 0.005). When either macrophages or CD4+ cells were depleted before administration of viral therapy, TK + Flt3L therapy failed to prolong survival. Meanwhile, depletion of CD8+ cells or natural killer cells did not affect TK + Flt3L efficacy. Spinal cord of animals surviving 6 months after TK + Flt3L were evaluated for the presence of autoimmune lesions. Whereas macrophages were present within the corticospinal tract and low levels of T-cell infiltration were detected, these effects are not indicative of an overt autoimmune disorder. We propose that combined Flt3L and HSV1-TK adenoviral-mediated gene therapy may provide an effective antiglioma treatment with increased efficacy in clinical trials of glioma.
Figures
References
-
- Counsell CE, Grant R. Incidence studies of primary and secondary intracranial tumors: a systematic review of their methodology and results. J Neurooncol. 1998;37:241–50. - PubMed
-
- Castro MG, Cowen R, Williamson IK, et al. Current and future strategies for the treatment of malignant brain tumors. Pharmacol Ther. 2003;98:71–108. - PubMed
-
- Dewey RA, Morrissey G, Cowsill CM, et al. Chronic brain inflammation and persistent herpes simplex virus 1 thymidine kinase expression in survivors of syngeneic glioma treated by adenovirus-mediated gene therapy: implications for clinical trials. Nat Med. 1999;5:1256–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
