

Idiopathic restrictive cardiomyopathy in children
- PMID: 16103558
- PMCID: PMC1769097
- DOI: 10.1136/hrt.2004.043869
Idiopathic restrictive cardiomyopathy in children
Abstract
Objective: To define the natural history of idiopathic restrictive cardiomyopathy in a paediatric population and to identify any factors predictive of outcome.
Design: Retrospective analysis of patients born between 1970 and 2002 were identified from the Children's Hospital of Pittsburgh cardiology database. Demographic data, mode of presentation, echocardiographic and haemodynamic findings at diagnosis, survival time, and manner of death were evaluated.
Setting: Tertiary referral and transplant centre for paediatric patients with cardiac disease.
Patients: All local and referred patients with idiopathic restrictive cardiomyopathy born after 1970 and under 21 years of age at time of diagnosis.
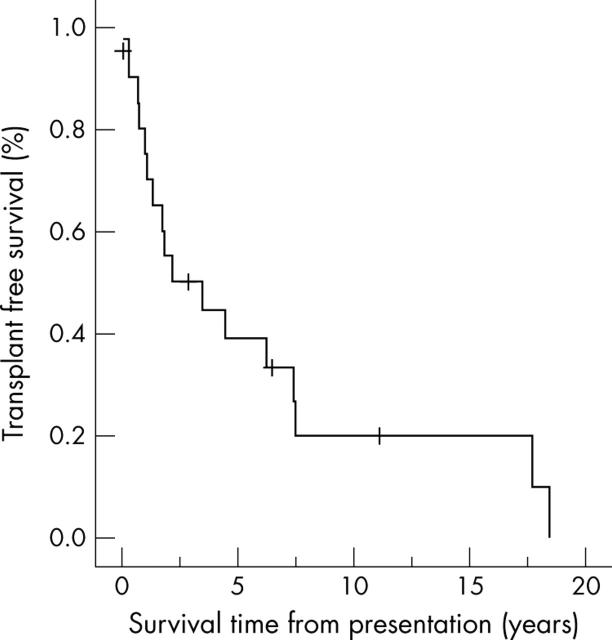
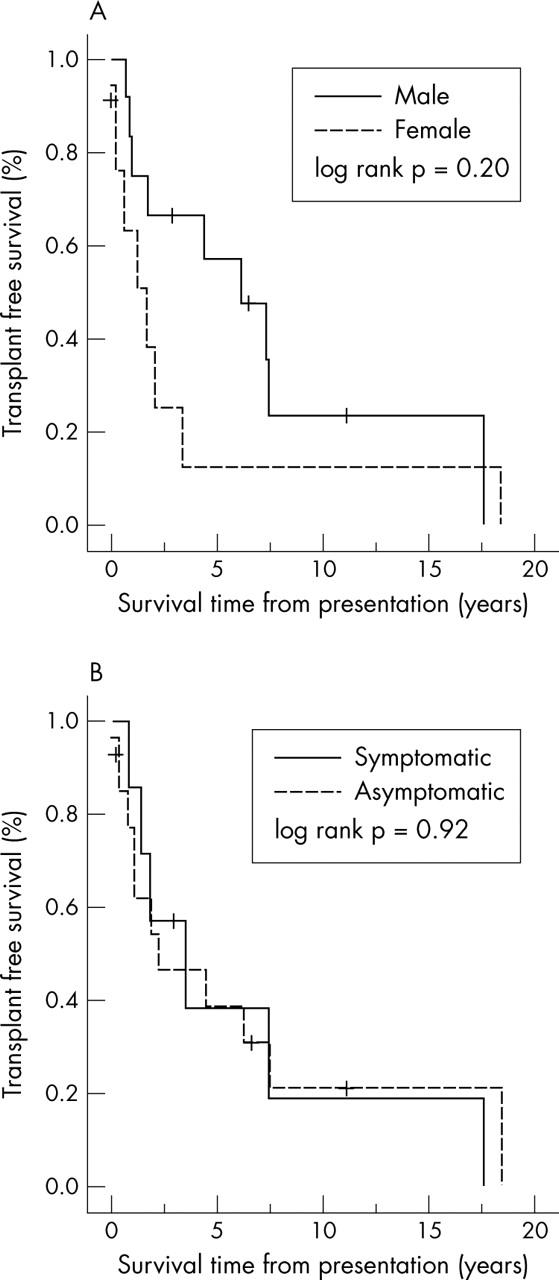
Results: 21 patients were identified. Probability of survival at 1, 5, and 10 years was 80.5% (95% confidence interval (CI) 58 to 100), 39% (95% CI 17 to 61), and 20% (95% CI 0 to 42), respectively. Median age of presentation was 3.8 years (mean (SD) 5.7 (6.1) years). Median survival without transplantation was 2.2 years (mean (SD) 4.6 (5.4) years). Age at presentation, sex, and presence or absence of heart failure symptoms at presentation were not associated with clinical course. Right (p = 0.05) and left ventricular end diastolic pressures (p = 0.04) and ratio of left atrial to aortic root dimensions (LA:Ao) (p = 0.03) at presentation had a significantly negative correlation with survival time after diagnosis.
Conclusions: Without transplantation, most children with restrictive cardiomyopathy have a very poor prognosis. Longer survival from diagnosis was correlated with lower LA:Ao and cardiac filling pressures at diagnosis. Survival time was not influenced by the symptoms present at diagnosis.
Figures
Similar articles
-
Conduction abnormalities in pediatric patients with restrictive cardiomyopathy.Circ Heart Fail. 2012 Mar 1;5(2):267-73. doi: 10.1161/CIRCHEARTFAILURE.111.964395. Epub 2012 Jan 19. Circ Heart Fail. 2012. PMID: 22260945
-
Heart and heart-lung transplantation for idiopathic restrictive cardiomyopathy in children.Heart. 2006 Jan;92(1):85-9. doi: 10.1136/hrt.2004.049502. Heart. 2006. PMID: 16365357 Free PMC article.
-
Outcomes of restrictive cardiomyopathy in childhood and the influence of phenotype: a report from the Pediatric Cardiomyopathy Registry.Circulation. 2012 Sep 4;126(10):1237-44. doi: 10.1161/CIRCULATIONAHA.112.104638. Epub 2012 Jul 27. Circulation. 2012. PMID: 22843787 Clinical Trial.
-
Restrictive cardiomyopathy.Pacing Clin Electrophysiol. 2009 Jul;32 Suppl 2:S41-3. doi: 10.1111/j.1540-8159.2009.02383.x. Pacing Clin Electrophysiol. 2009. PMID: 19602161 Review.
-
[Idiopathic dilated cardiomyopathies in children. Development and prognostic factors].Arch Mal Coeur Vaiss. 1991 May;84(5):721-6. Arch Mal Coeur Vaiss. 1991. PMID: 1898208 Review. French.
Cited by
-
A case of restrictive cardiomyopathy complicated by recurrent pulmonary thromboembolism originating at the right atrial appendage.J Cardiol Cases. 2020 Mar 28;21(6):220-223. doi: 10.1016/j.jccase.2020.02.004. eCollection 2020 Jun. J Cardiol Cases. 2020. PMID: 32547657 Free PMC article.
-
The 'Padua classification' of cardiomyopathies into three groups: hypertrophic/restrictive, dilated/hypokinetic, and scarring/arrhythmogenic.Eur Heart J Suppl. 2025 Feb 19;27(Suppl 1):i73-i82. doi: 10.1093/eurheartjsupp/suae108. eCollection 2025 Feb. Eur Heart J Suppl. 2025. PMID: 39980775 Free PMC article.
-
Insights into restrictive cardiomyopathy from clinical and animal studies.J Geriatr Cardiol. 2011 Sep;8(3):168-83. doi: 10.3724/SP.J.1263.2011.00168. J Geriatr Cardiol. 2011. PMID: 22783303 Free PMC article.
-
Pediatric cardiomyopathies: causes, epidemiology, clinical course, preventive strategies and therapies.Future Cardiol. 2013 Nov;9(6):817-48. doi: 10.2217/fca.13.66. Future Cardiol. 2013. PMID: 24180540 Free PMC article. Review.
-
Overview of Cardiomyopathies in Childhood.Front Pediatr. 2021 Jul 23;9:708732. doi: 10.3389/fped.2021.708732. eCollection 2021. Front Pediatr. 2021. PMID: 34368032 Free PMC article. Review.
References
-
- Nuget AW, Daubeney P, Chondros P, et al. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med 2003;248:1639–46. - PubMed
-
- Lipschutz SE, Sleeper LA, Towbin JA, et al. The incidence of pediatric cardiomyopathy in two regions of the United States. N Engl J Med 2003;348:1647–55. - PubMed
-
- Malcic I, Jelusic M, Kniewald H, et al. Epidemiology of cardiomyopathies in children and adolescents: a retrospective study. Cardiol Young 2002;12:253–9. - PubMed
-
- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology task force on the definition and classification of cardiomyopathies. Circulation 1996;93:841–2. - PubMed
-
- Chen S, Balfour IC, Jureidini S. Clinical spectrum of restrictive cardiomyopathy in children. J Heart Lung Transplant 2001;20:90–2. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources