

Interruption of aortic arch in adults: surgical experience with extra-anatomic bypass
- PMID: 16107103
- PMCID: PMC1163459
Interruption of aortic arch in adults: surgical experience with extra-anatomic bypass
Abstract
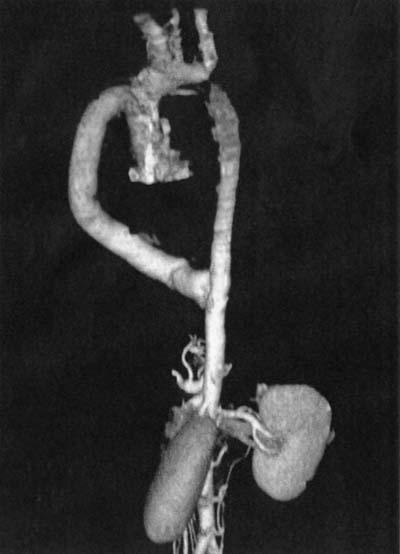
We reviewed our 3-year experience in treating interruption of the aorta in adult patients. Clinical profiles, surgical management, and results of early and mid-term follow-up are presented. From August 2001 through June 2003, 7 adult patients underwent an extra-anatomic bypass procedure to repair interruption of the aortic arch. Five patients underwent ventral aortic repair through a mid-sternotomy and an upper midline laparotomy, and 2 patients underwent repair through a left posterolateral thoracotomy. A bovine collagen-impregnated polyester fiber graft was used in 6 patients, and a Gore-Tex graft was interposed in 1 patient. All repairs were performed without cardiopulmonary bypass. Follow-up was complete in all patients. The mean follow-up was 1728 +/- 1 months (range, 9-31 months). No neurologic, renal, or gastrointestinal complications were noted in any patient. There was no in-hospital or late mortality or need for re-intervention. All patients were asymptomatic; however, 5 patients had mild residual hypertension. Graft patency in all the patients was confirmed by computed tomographic angiography. Interruption of the aorta is rare in adults. Ventral aortic repair through a midline approach is our preferred technique for surgical repair of this entity, because it avoids the extensive network of collateral vessels on the chest wall, enables simultaneous treatment of associated lesions, and in all likelihood reduces morbidity and mortality.
Figures

Similar articles
-
Congenital native interruption of aortic arch in an adult: extra-anatomic approach by right-side thoracotomy.J Vasc Surg. 2010 Jun;51(6):1525-7. doi: 10.1016/j.jvs.2010.01.055. Epub 2010 Apr 10. J Vasc Surg. 2010. PMID: 20385466
-
Interrupted aortic arch in an adult single-stage extra-anatomic repair.Tex Heart Inst J. 2002;29(2):118-21. Tex Heart Inst J. 2002. PMID: 12075868 Free PMC article. Review.
-
Surgical conversion after thoracic endovascular aortic repair.J Thorac Cardiovasc Surg. 2011 Nov;142(5):1027-31. doi: 10.1016/j.jtcvs.2011.01.060. Epub 2011 Mar 12. J Thorac Cardiovasc Surg. 2011. PMID: 21397263
-
Posterior pericardial ascending-to-descending aortic bypass through median sternotomy.J Card Surg. 2008 Sep-Oct;23(5):515-8. doi: 10.1111/j.1540-8191.2008.00582.x. Epub 2008 May 7. J Card Surg. 2008. PMID: 18462343
-
Outcomes in patients with interrupted aortic arch and associated anomalies: a 20-year experience.Eur J Cardiothorac Surg. 2006 May;29(5):666-73; discussion 673-4. doi: 10.1016/j.ejcts.2006.01.060. Epub 2006 Apr 12. Eur J Cardiothorac Surg. 2006. PMID: 16626964 Review.
Cited by
-
Interrupted aortic arch with severe aortic stenosis in an adult bicuspid aortic valve patient.Indian J Thorac Cardiovasc Surg. 2025 Apr;41(4):464-467. doi: 10.1007/s12055-024-01828-0. Epub 2024 Sep 23. Indian J Thorac Cardiovasc Surg. 2025. PMID: 40144607
-
Interrupted aortic arch diagnosis by computed tomography angiography and 3-D reconstruction: A case report.Radiol Case Rep. 2017 Nov 17;13(1):35-38. doi: 10.1016/j.radcr.2017.10.001. eCollection 2018 Feb. Radiol Case Rep. 2017. PMID: 29552241 Free PMC article.
-
Discontinuity of the arch beyond the origin of the left subclavian artery in an adult: Interruption or coarctation?Ann Pediatr Cardiol. 2018 Jan-Apr;11(1):92-96. doi: 10.4103/apc.APC_91_17. Ann Pediatr Cardiol. 2018. PMID: 29440839 Free PMC article.
-
Asymptomatic Interrupted Aortic Arch, Severe Tricuspid Regurgitation, and Bicuspid Aortic Valve in a 76-Year-Old Woman.Tex Heart Inst J. 2016 Oct 1;43(5):437-440. doi: 10.14503/THIJ-15-5320. eCollection 2016 Oct. Tex Heart Inst J. 2016. PMID: 27777532 Free PMC article. Review.
-
4-D MRI flow analysis in the course of interrupted aortic arch reveals complex morphology and quantifies amount of collateral blood flow.Pediatr Radiol. 2013 Aug;43(8):1037-40. doi: 10.1007/s00247-013-2641-1. Epub 2013 Feb 17. Pediatr Radiol. 2013. PMID: 23417233
References
-
- Siderys H, Graffis R, Halbrook H, Kasbeckar V. A technique for management of inaccessible coarctation of the aorta. J Thorac Cardiovasc Surg 1974;67:568–70. - PubMed
-
- Wukasch DC, Cooley DA, Sandiford FM, Nappi G, Reul GJ Jr. Ascending aorta-abdominal aorta bypass: indications, technique, and report of 12 patients. Ann Thorac Surg 1977;23:442–8. - PubMed
-
- Robicsek F, Hess PJ, Vajtai P. Ascending-distal abdominal aorta bypass for treatment of hypoplastic aortic arch and atypical coarctation in the adult. Ann Thorac Surg 1984; 37:261–3. - PubMed
-
- Steidele RJ. Samml Chir U Med Beob (Vienna) 1778;2: 114.
-
- Celoria GC, Patton RB. Congenital absence of the aortic arch. Am Heart J 1959;58:407–13. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical