

Sex and racial differences in the management of acute myocardial infarction, 1994 through 2002
- PMID: 16107620
- PMCID: PMC2805130
- DOI: 10.1056/NEJMsa032214
Sex and racial differences in the management of acute myocardial infarction, 1994 through 2002
Abstract
Background: Although increased attention has been paid to sex and racial differences in the management of myocardial infarction, it is unknown whether these differences have narrowed over time.
Methods: With the use of data from the National Registry of Myocardial Infarction, we examined sex and racial differences in the treatment of patients who were deemed to be "ideal candidates" for particular treatments and in deaths among 598,911 patients hospitalized with myocardial infarction between 1994 and 2002.
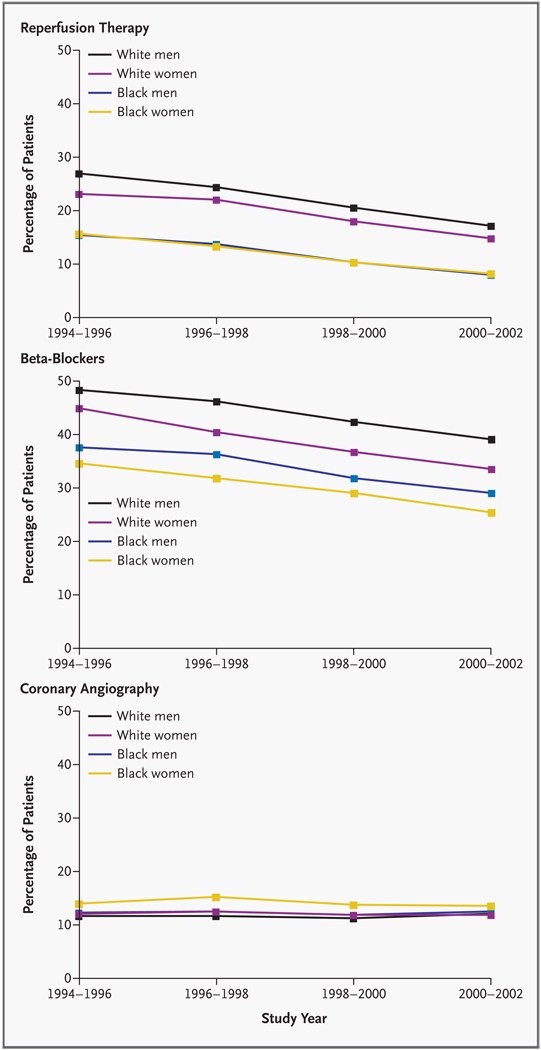
Results: In the unadjusted analysis, sex and racial differences were observed for rates of reperfusion therapy (for white men, white women, black men, and black women: 86.5, 83.3, 80.4, and 77.8 percent, respectively; P<0.001), use of aspirin (84.4, 78.7, 83.7, and 78.4 percent, respectively; P<0.001), use of beta-blockers (66.6, 62.9, 67.8, and 64.5 percent; P<0.001), and coronary angiography (69.1, 55.9, 64.0, and 55.0 percent; P<0.001). After multivariable adjustment, racial and sex differences persisted for rates of reperfusion therapy (risk ratio for white women, black men, and black women: 0.97, 0.91, and 0.89, respectively, as compared with white men) and coronary angiography (relative risk, 0.91, 0.82, and 0.76) but were attenuated for the use of aspirin (risk ratio, 0.97, 0.98, and 0.94) and beta-blockers (risk ratio, 0.98, 1.00, and 0.96); all risks were unchanged over time. Adjusted in-hospital mortality was similar among white women (risk ratio, 1.05; 95 percent confidence interval, 1.03 to 1.07) and black men (risk ratio, 0.95; 95 percent confidence interval, 0.89 to 1.00), as compared with white men, but was higher among black women (risk ratio, 1.11; 95 percent confidence interval, 1.06 to 1.16) and was unchanged over time.
Conclusions: Rates of reperfusion therapy, coronary angiography, and in-hospital death after myocardial infarction, but not the use of aspirin and beta-blockers, vary according to race and sex, with no evidence that the differences have narrowed in recent years.
Copyright 2005 Massachusetts Medical Society.
Figures
Comment in
-
Health disparities--less talk, more action.N Engl J Med. 2005 Aug 18;353(7):727-9. doi: 10.1056/NEJMe058143. N Engl J Med. 2005. PMID: 16107626 No abstract available.
-
Trends in racial disparities in care.N Engl J Med. 2005 Nov 10;353(19):2081-5; author reply 2081-5. doi: 10.1056/NEJM200511103531918. N Engl J Med. 2005. PMID: 16282186 No abstract available.
-
Trends in racial disparities in care.N Engl J Med. 2005 Nov 10;353(19):2081-5; author reply 2081-5. N Engl J Med. 2005. PMID: 16285158 No abstract available.
References
-
- Ayanian JZ, Epstein AM. Differences in the use of procedures between women and men hospitalized for coronary heart disease. N Engl J Med. 1991;325:221–225. - PubMed
-
- Steingart RM, Packer M, Hamm P, et al. Sex differences in the management of coronary artery disease. N Engl J Med. 1991;325:226–230. - PubMed
-
- Wenneker MB, Epstein AM. Racial inequalities in the use of procedures for patients with ischemic heart disease in Massachusetts. JAMA. 1989;261:253–257. - PubMed
-
- Whittle J, Conigliaro J, Good CB, Lofgren RP. Racial differences in the use of invasive cardiovascular procedures in the Department of Veterans Affairs medical system. N Engl J Med. 1993;329:621–627. - PubMed
-
- Yarzebski J, Col N, Pagley P, Savageau J, Gore J, Goldberg R. Gender differences and factors associated with the receipt of thrombolytic therapy in patients with acute myocardial infarction: a community-wide perspective. Am Heart J. 1996;131:43–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical