

Anti-platelet factor 4/heparin antibodies in orthopedic surgery patients receiving antithrombotic prophylaxis with fondaparinux or enoxaparin
- PMID: 16109780
- PMCID: PMC1895104
- DOI: 10.1182/blood-2005-05-1938
Anti-platelet factor 4/heparin antibodies in orthopedic surgery patients receiving antithrombotic prophylaxis with fondaparinux or enoxaparin
Abstract
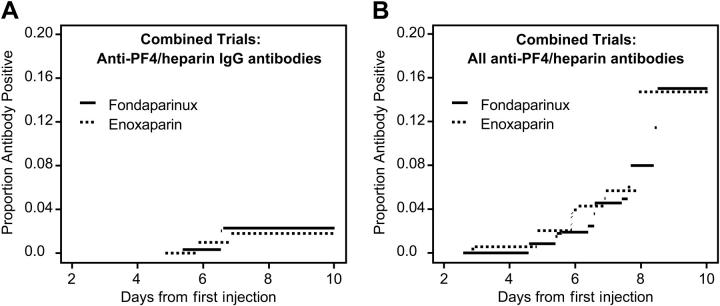
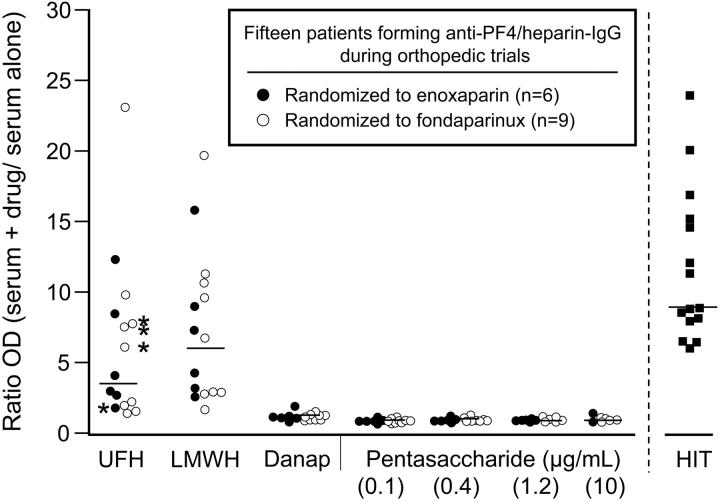
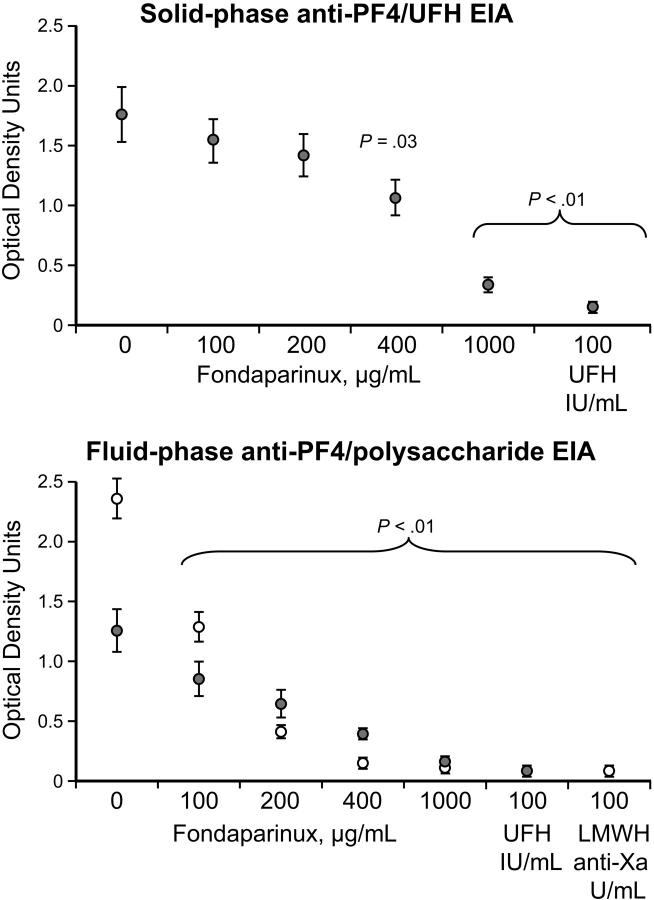
Heparin-induced thrombocytopenia (HIT) is caused by platelet-activating IgG antibodies that recognize platelet factor 4 (PF4) bound to heparin. Immunogenicity of heparins differs in that unfractionated heparin (UFH) induces more anti-PF4/heparin antibodies than low-molecular-weight heparin (LMWH) and UFH also causes more HIT. Fondaparinux, a synthetic anticoagulant modeled after the antithrombin-binding pentasaccharide, is believed to be nonimmunogenic. We tested 2726 patients for anti-PF4/heparin antibodies after they were randomized to receive antithrombotic prophylaxis with fondaparinux or LMWH (enoxaparin) following hip or knee surgery. We also evaluated in vitro cross-reactivity of the IgG antibodies generated against PF4 in the presence of UFH, LMWH, danaparoid, or fondaparinux. We found that anti-PF4/heparin antibodies were generated at similar frequencies in patients treated with fondaparinux or enoxaparin. Although antibodies reacted equally well in vitro against PF4/UFH and PF4/LMWH, and sometimes weakly against PF4/danaparoid, none reacted against PF4/fondaparinux, including even those sera obtained from patients who formed antibodies during fondaparinux treatment. At high concentrations, however, fondaparinux inhibited binding of HIT antibodies to PF4/polysaccharide, indicating that PF4/fondaparinux interactions occur. No patient developed HIT. We conclude that despite similar immunogenicity of fondaparinux and LMWH, PF4/fondaparinux, but not PF4/LMWH, is recognized poorly by the antibodies generated, suggesting that the risk of HIT with fondaparinux likely is very low.
Figures
References
-
- Lormeau JC, Herault JP. The effect of the synthetic pentasaccharide SR 90107/ORG 31540 on thrombin generation ex vivo is uniquely due to ATIII-mediated neutralization of factor Xa. Thromb Haemost. 1995;74: 1474-1477. - PubMed
-
- Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin for the prevention of venous thromboembolism in major orthopedic surgery: a meta-analysis of 4 randomized double-blind studies. Arch Intern Med. 2002;162: 1833-1840. - PubMed
-
- Büller HR, Davidson BL, Decousus H, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis. Ann Intern Med. 2004;140: 867-873. - PubMed
-
- Matisse Investigators. Subcutaneous fondaparinux versus intravenous unfractionated heparin in the initial treatment of pulmonary embolism. N Engl J Med. 2003;349: 1695-1702. - PubMed
-
- Aster RH. Heparin-induced thrombocytopenia and thrombosis. N Engl J Med. 1995;332: 1374-1376. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
