

Outcome of asthma and wheezing in the first 6 years of life: follow-up through adolescence
- PMID: 16109980
- PMCID: PMC2718414
- DOI: 10.1164/rccm.200504-525OC
Outcome of asthma and wheezing in the first 6 years of life: follow-up through adolescence
Abstract
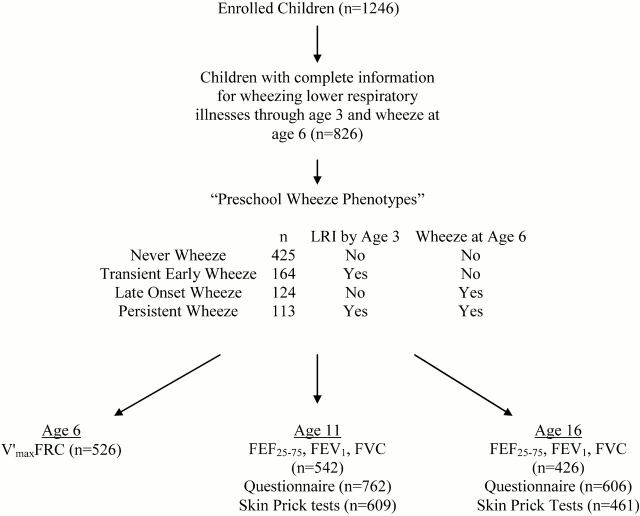
Rationale: The effect of early life wheezing on respiratory function and continued symptoms through adolescence has not been fully described. Using data from a population-based birth cohort in Tucson, Arizona, we previously described four phenotypes based on the occurrence of wheezing lower respiratory illnesses before age 3 yr and active wheeze at age 6 yr: never wheezers (n = 425), transient early wheezers (n = 164), persistent wheezers (n = 113), and late-onset wheezers (n = 124).
Objective: We sought to determine the prognosis for these phenotypes, with reference to lung function and symptoms, through adolescence.
Methods: Current wheeze was assessed by questionnaire, lung function was measured by conventional spirometry, and atopy was determined by skin prick tests.
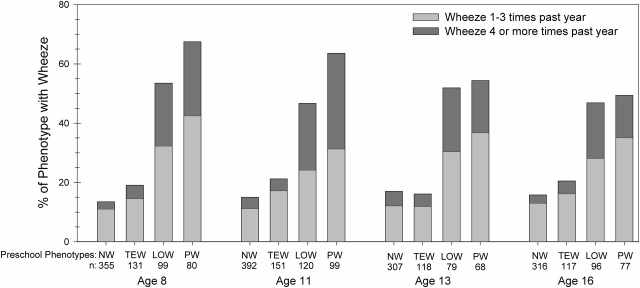
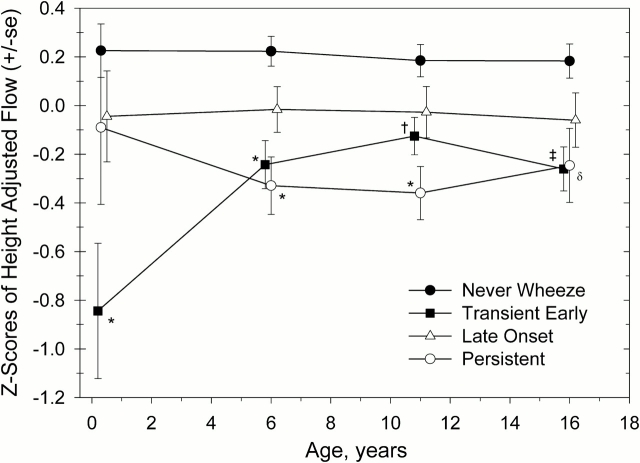
Results: The prevalence of atopy and wheeze by age 16 yr was similar for never and transient wheezers and for persistent and late-onset wheezers. Both transient early, and persistent wheezers had significantly lower FEF(25-75) (-259 ml/s, p < 0.001, and -260 ml/s, p = 0.001, respectively), FEV1 (-75 ml, p = 0.02, and -87 ml, p = 0.03, respectively), and FEV1:FVC ratio (-1.9%, p = 0.002, and -2.5%, p = 0.001, respectively) through age 16 yr compared with never wheezers. Late-onset wheezers had levels of lung function similar to those of never wheezers through age 16 yr. There was no significant change in lung function among subjects with any of the four phenotypes, relative to their peers, from age 6 to 16 yr.
Conclusion: Patterns of wheezing prevalence and levels of lung function are established by age 6 yr and do not appear to change significantly by age 16 yr in children who start having asthma-like symptoms during the preschool years.
Figures
Comment in
-
Does most asthma really begin during the preschool years?Am J Respir Crit Care Med. 2006 Mar 1;173(5):575-6; author reply 576. doi: 10.1164/ajrccm.173.5.575. Am J Respir Crit Care Med. 2006. PMID: 16493166 No abstract available.
References
-
- Martinez FD. Toward asthma prevention: does all that really matters happen before we learn to read? N Engl J Med 2003;349:1473–1475. - PubMed
-
- Martinez FD, Godfrey S. Wheezing disorders in the preschool child. London: Martin Dunitz, Taylor & Francis Group; 2003.
-
- Phelan PD, Robertson CF, Olinsky A. The Melbourne Asthma Study: 1964–1999. J Allergy Clin Immunol 2002;109:189–194. - PubMed
-
- Sears MR, Greene JM, Willan AR, Wiecek EM, Taylor DR, Flannery EM, Cowan JO, Herbison GP, Silva PA, Poulton R. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N Engl J Med 2003;349:1414–1422. - PubMed
-
- Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ, Group Health Medical Associates. Asthma and wheezing in the first six years of life. N Engl J Med 1995;332:133–138. - PubMed
