

Anti-SARS-CoV IgG response in relation to disease severity of severe acute respiratory syndrome
- PMID: 16112612
- PMCID: PMC7108264
- DOI: 10.1016/j.jcv.2005.07.005
Anti-SARS-CoV IgG response in relation to disease severity of severe acute respiratory syndrome
Abstract
Background: The association between a robust or depressed antibody response and clinical severity of SARS remains unknown.
Objectives: To study seroconversion and the magnitude of IgG responses in a SARS cohort with different disease severities.
Study design and method: A retrospective analysis of all acute and convalescent-phase sera collected from a cohort of laboratory-confirmed SARS cases. Anti-SARS-CoV IgG antibody was detected using indirect immunofluorescence technique and quantified by two-fold serial dilutions. Characteristics of patients who seroconverted "early" (<median interval) were compared to those documented to remain sero-negative during the same time interval. Median IgG levels in convalescent-phase sera (collected within 30 days) were compared among patients with different disease severities. Correlations between IgG levels and important laboratory parameters were assessed.
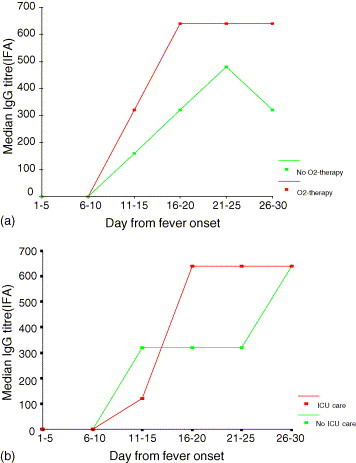
Results: A total of 325 laboratory-confirmed SARS cases were analyzed; of which 301 (92.6%) had anti-SARS-CoV IgG detected in their sera at the time of sampling. IgG was first detected on day 4 of illness; seroconversion occurred at a median of 16 days (range 4-35 days), and IgG peak levels were reached in the fourth week. Early seroconversion (<day 16) occurred more frequently among patients who required ICU-admission (chi2; p=0.011). Higher IgG levels were detected in patients who required supplemental oxygen (Mann-Whitney; p=0.002), ICU-admission (p=0.001), had negative pre-discharge fecal RT-PCR results (p=0.004), and lymphopenia at presentation (p=0.028). Peak IgG titres also correlated positively with peak LDH levels (Spearman's r=+0.360; p<0.001) among survivors.
Conclusions: Severe SARS is associated with a more robust IgG response.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). Severe acute respiratory syndrome (SARS). http://www.cdc.gov/ncidod/sars/lab/biosafety.htm.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
