

Outcomes of high volume cataract surgeries in a developing country
- PMID: 16113352
- PMCID: PMC1772816
- DOI: 10.1136/bjo.2004.063479
Outcomes of high volume cataract surgeries in a developing country
Abstract
Aim: To analyse the outcome of high volume cataract surgery in a developing country, community based, high volume eye hospital.
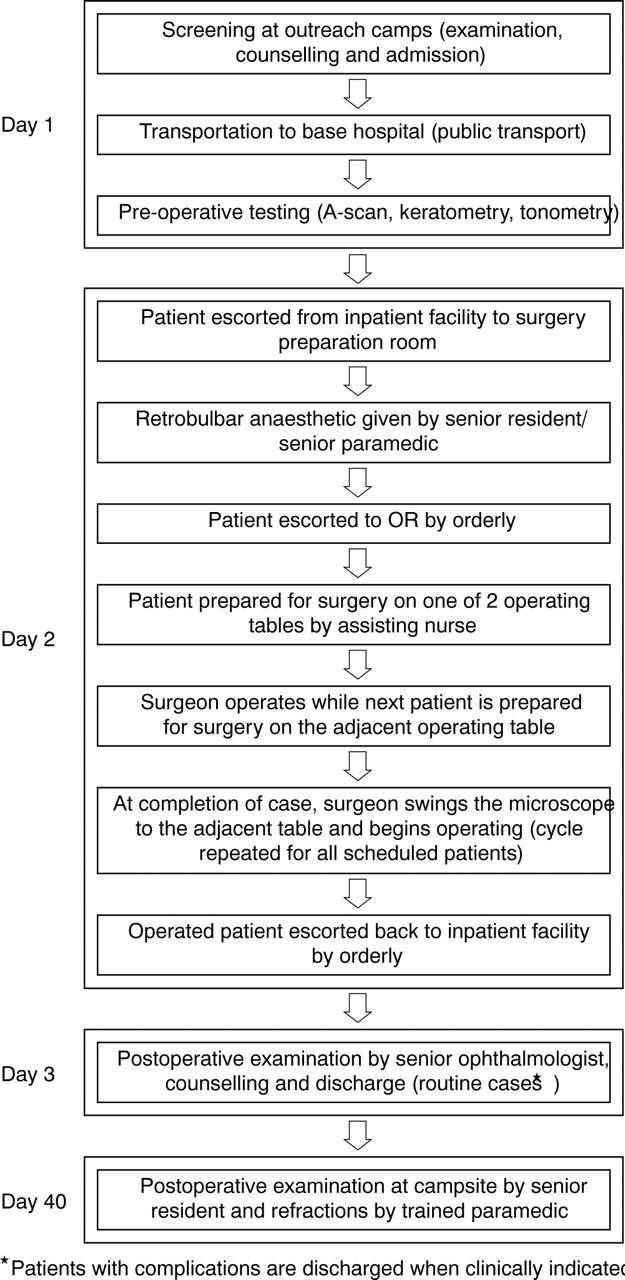
Methods: In a non-comparative interventional case series, the authors reviewed the surgical outcomes of 593 patients with cataract operated upon by three high volume surgeons on six randomly selected days. There were 318 female (54%) and 275 male (46%) patients. Their mean age was 59.57 (SD 10.13) years. The majority of the patients underwent manual small incision cataract surgery (manual SICS). Extracapsular cataract extraction with posterior chamber intraocular lens (ECCE-PCIOL) and intracapsular cataract extraction (ICCE) were also done on a few patients as clinically indicated.
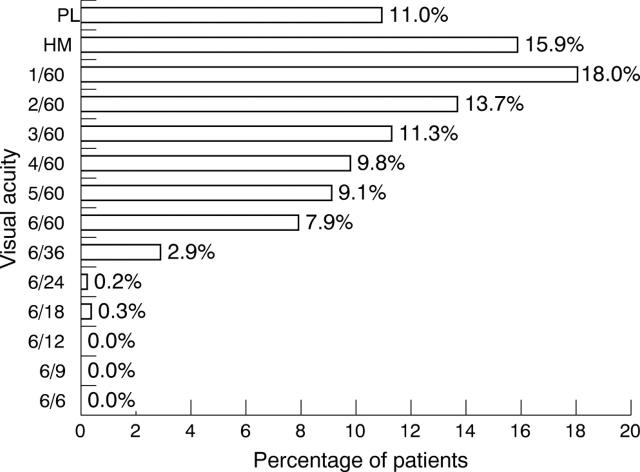
Results: Best corrected visual acuity of >or=6/18 was achieved in 94% of the 520 patients who could be followed up on the 40th postoperative day (88% follow up rate). Intraoperative and immediate postoperative complications as defined by OCTET occurred in 11 (1.9%) and 75 (12.6%) patients, respectively. Average surgical time of 3.75 minutes per case (16-18 cases per hour) was achieved. Statistically significant risk factors for outcomes were found to be age >60, sex, and surgeon.
Conclusion: High volume surgery using appropriate techniques and standardised protocols does not compromise quality of outcomes.
Figures
References
-
- Jose R . National programme for control of blindness. Indian J Commun Health 1997;3:5–9.
-
- Dandona L , Dandona R, Naduvilath T, et al. Is the current eye-care policy focus almost exclusively on cataract adequate to deal with blindness in India? Lancet 1998;351:1312–16. - PubMed
-
- Dandona L , Dandona R, Anand R, et al. Outcome and number of cataract surgeries in India: policy issues for blindness control. Clin Experiment Ophthalmol 2003;31:23–31. - PubMed
-
- Natchiar G , Robin AL, Ravilla D, et al. Attacking the backlog of India’s curable blind. Arch Ophthalmol 1994;112:987–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources