

Levels of prostaglandin E metabolite, the major urinary metabolite of prostaglandin E2, are increased in smokers
- PMID: 16115954
- PMCID: PMC1939807
- DOI: 10.1158/1078-0432.CCR-05-0733
Levels of prostaglandin E metabolite, the major urinary metabolite of prostaglandin E2, are increased in smokers
Abstract
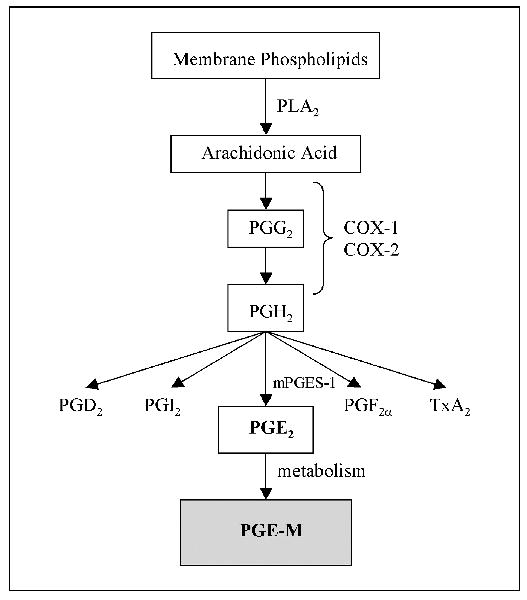
Purpose: Increased levels of cyclooxygenase-2 and prostaglandin E2 (PGE2) have been observed in tobacco-related malignancies of the upper aerodigestive tract. Moreover, exposure to tobacco smoke can stimulate the synthesis of PGE2. Recent evidence suggests that urinary PGE metabolite (PGE-M) can be used as an index of systemic PGE2 production. In this study, we investigated whether levels of urinary PGE-M were increased in smokers and in patients with head and neck squamous cell carcinoma (HNSCC).
Experimental design: Fifty-eight HNSCC cases and 29 age- and gender-matched healthy controls were prospectively enrolled in the study. A detailed smoking history and single void urine specimen were obtained from each participant. Levels of urinary PGE-M were quantified in a blinded fashion using mass spectrometry and compared with smoking history and tumor status.
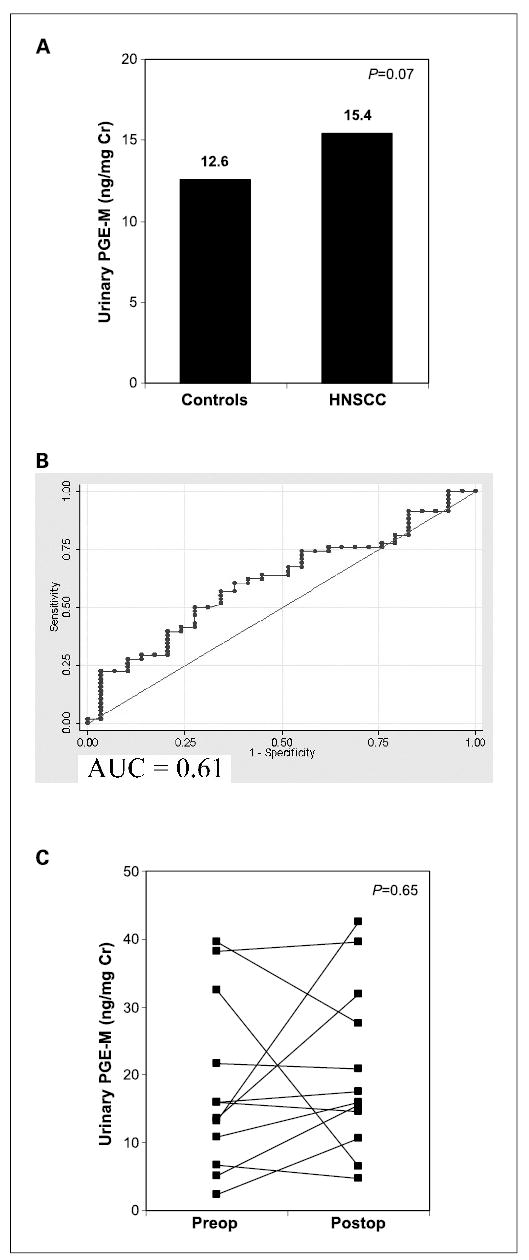
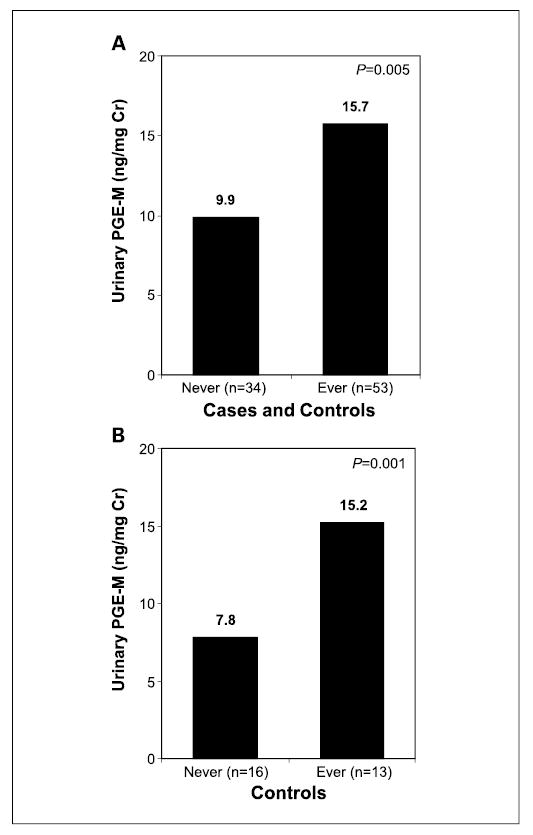
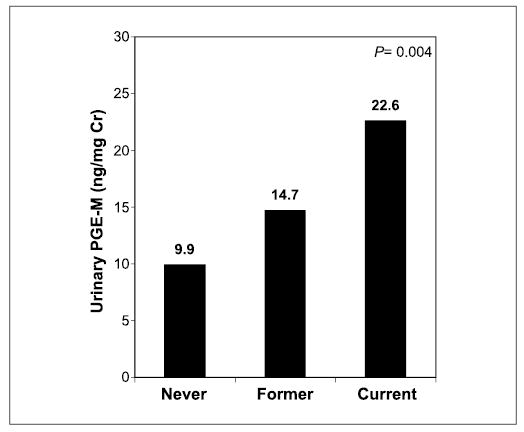
Results: Adjusted for case-control matching, median urinary PGE-M levels were significantly higher in ever smokers (15.7 ng/mg creatinine) compared with never smokers (9.9 ng/mg creatinine) for the entire study population (n = 87, P = 0.005). Concentrations of urinary PGE-M were nearly doubled in ever smokers (15.2 ng/mg creatinine) versus never smokers (7.8 ng/mg creatinine) among healthy controls (P = 0.001). Higher PGE-M levels were observed in current versus former smokers and in those with greater pack-year exposure. A significant difference in amounts of PGE-M was not observed in patients with HNSCC versus healthy controls.
Conclusions: Increased levels of urinary PGE-M were observed in smokers. Urinary PGE-M may have use as a noninvasive biomarker of the effects of tobacco smoke exposure.
Figures
References
-
- Lewin F, Norell SE, Johansson H, et al. Smoking tobacco, oral snuff, and alcoholin the etiology of squamous cell carcinoma of the head and neck: a population-based case-referent study in Sweden. Cancer. 1998;82:1367–75. - PubMed
-
- Mashberg A, Boffetta P, Winkelman R, Garfinkel L. Tobacco smoking, alcohol drinking, and cancer of the oral cavity and oropharynx among U.S. veterans. Cancer. 1993;72:1369–75. - PubMed
-
- Vineis P, Alavanja M, Buffler P, et al. Tobacco and cancer: recent epidemiological evidence. J Natl Cancer Inst. 2004;96:99–106. - PubMed
-
- DeMarini DM. Genotoxicity of tobacco smoke and tobacco smoke condensate: a review. Mutat Res. 2004;567:447–74. - PubMed
-
- Izzotti A, Cartiglia C, Longobardi M, et al. Gene expression in the lung of p53 mutant mice exposed to cigarette smoke. Cancer Res. 2004;64:8566–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 CA09685/CA/NCI NIH HHS/United States
- P01 CA106451/CA/NCI NIH HHS/United States
- R01 DK048831/DK/NIDDK NIH HHS/United States
- P01 CA77839/CA/NCI NIH HHS/United States
- P01 CA077839/CA/NCI NIH HHS/United States
- T32 CA009685/CA/NCI NIH HHS/United States
- P50 GM015431/GM/NIGMS NIH HHS/United States
- R01 DK48831/DK/NIDDK NIH HHS/United States
- RR00095/RR/NCRR NIH HHS/United States
- R01 CA082578/CA/NCI NIH HHS/United States
- M01 RR000095/RR/NCRR NIH HHS/United States
- R01 CA82578/CA/NCI NIH HHS/United States
- P50GM15431/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
