

The impact of slow rewarming on inotropy, tissue metabolism, and "after drop" of body temperature in pediatric patients
- PMID: 16117455
- PMCID: PMC4682534
The impact of slow rewarming on inotropy, tissue metabolism, and "after drop" of body temperature in pediatric patients
Abstract
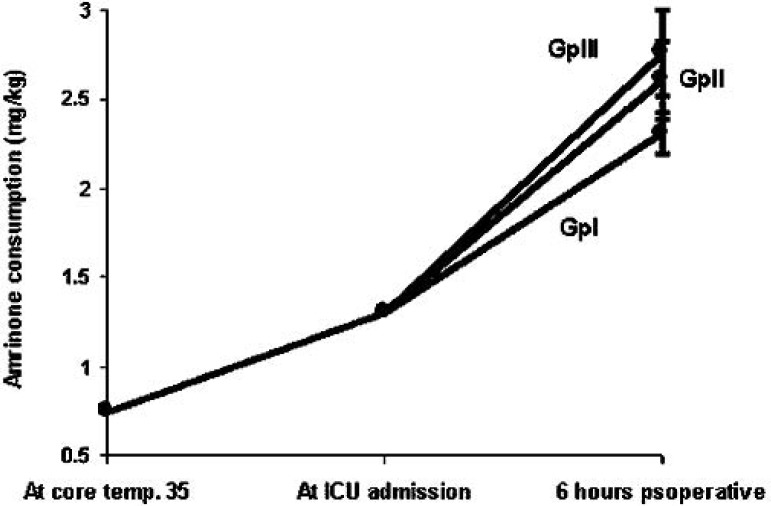
Pediatric patients undergoing surgical correction of congenital heart diseases using cardiopulmonary bypass (CPB) are subjected to hypothermia. Core temperature is cooled down to 26-28 degrees C during CPB. Postoperative hypothermia in these patients remains a source of long-intensive care unit (ICU) stay. Therefore, this study was performed to build a rewarming strategy aiming to improve the cardiac performance, minimize the early after-drop in both core and foot temperatures, and to achieve early achievement of homeostasis. Thirty pediatric patients of acyanotic congenital heart diseases were randomly allocated into one of three equal groups of 10. Group I was kept at 3 degrees C between nasopharyngeal and heater-cooler unit water temperatures during rewarming whereas group II and group III were kept at 5 degrees C and 7 degrees C, respectively. The following parameters were measured: 1) cardiac performance (cardiac index and peak velocity); 2) cumulative amrinone consumption, blood lactate levels, and total body oxygen consumption; 3) intraoperative and postoperative peak and trough core and foot temperatures; and 4) time to extubation and ICU stay. Group I patients showed statistically significant increase in cardiac index and peak velocity compared with groups II and III, at p < 0.05 and p < 0.025, respectively. Statistically, the consumption of amrinone was significantly decreased in group I compared with groups II and III, with p < 0.005 and p < 0.0005, respectively, at 6 hours postoperatively. Group I showed an insignificant increase in blood lactate level, where groups II and III showed significant increases compared with controls (p < 0.001 at 6 hours postoperatively). Intraoperatively, both trough core and peak foot temperatures of group I patients statistically were significantly higher than in group III patients at p < 0.0005 and p < 0.05, respectively. The same applies in the ICU as regards to the time to core temperature (p < 0.005) and the rate of foot warming (p < 0.01). It was found that a difference of 3 degrees C (group I) between nasopharyngeal and heater-cooler unit water temperatures during rewarming demonstrated the best outcome compared with 5 degrees C and 7 degrees C differences (groups II and III, respectively). This outcome was obvious in the following parameters: 1) the best cardiac performance (cardiac index and peak velocity); 2) the lowest values of cumulative amrinone consumption and blood lactate level; 3) the least after-drop in both core and foot temperatures; and 4) achievement of early homeostasis, shortest ICU stays, and conservation of the ICU resources.
Conflict of interest statement
The senior author has stated that authors have reported no material, financial or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures



References
-
- Bisonnette B, Davis PJ.. Thermal regulation-physiology and perioperative management in infants and children. In: Ed Motoyama EK, Avis PJ eds. Smith’s Anesthesia for Infants and Children. St. Louis: Mosby-Year Book; 1996;139–158.
-
- Bissonnette B, Sessler DI.. Thermoregulatory thresholds for vasoconstriction in pediatric patients anesthetized with halothane or isoflurane and caudal bupivacaine. Anesthesiology. 1992;76:387. - PubMed
-
- Plattner O, Semsroth M, Sessler DI, Papousek A, Klasen C, Wagner O.. Lack of nonshivering thermogenesis in infants anesthetized with fentanyl and propofol. Anesthesiology. 1997;86:772–7. - PubMed
-
- Spaniol SE, Bond EF, Brengelmann GL, Savage M, Pozos RS.. Shivering following cardiac surgery: predictive factors, consequences and characteristics. Am J Crit Care. 1994;3:356–67. - PubMed
-
- Ramsay JG, Ralley FE, Whalley DG, Delli Colli P, Wynands JE.. Site of temperature monitoring and prediction of after drop after open heart surgery. Can Anaesth Soc J. 1985;32:607–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources