

Neoadjuvant chemotherapy versus primary surgery in advanced ovarian carcinoma
- PMID: 16135251
- PMCID: PMC1236969
- DOI: 10.1186/1477-7819-3-57
Neoadjuvant chemotherapy versus primary surgery in advanced ovarian carcinoma
Abstract
Background: Patients with advanced ovarian cancer should be treated by radical debulking surgery aiming at complete tumor resection. Unfortunately about 70% of the patients present with advanced disease, when optimal debulking can not be obtained, and therefore these patients gain little benefit from surgery. Neoadjuvant chemotherapy (NACT) has been proposed as a novel therapeutic approach in such cases. In this study, we report our results with primary surgery or neoadjuvant chemotherapy as treatment modalities in the specific indication of operable patients with advanced ovarian carcinoma (no medical contraindication to debulking surgery).
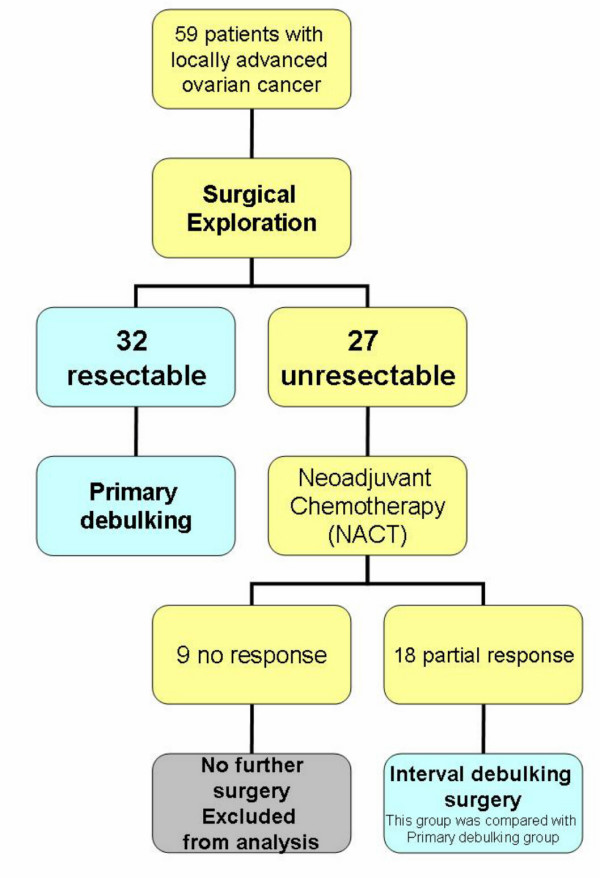
Patients and methods: A total of 59 patients with stage III or IV epithelial ovarian carcinomas were evaluated between 1998 and 2003. All patients were submitted to surgical exploration aiming to evaluate tumor resectability. Neoadjuvant chemotherapy was given (in 27 patients) where optimal cytoreduction was not feasible. Conversely primary debulking surgery was performed when we considered that optimal cytoreduction could be achieved by the standard surgery (32 patients).
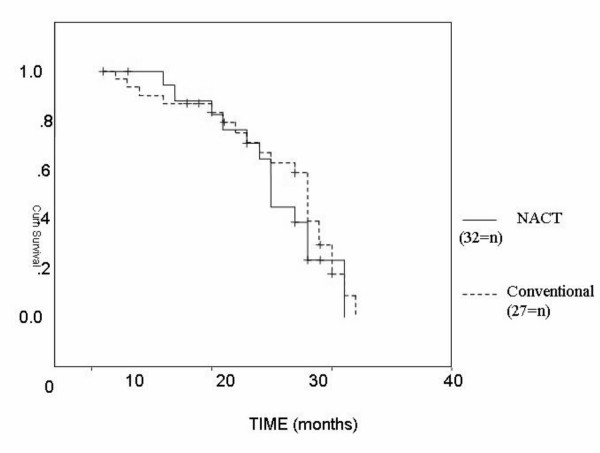
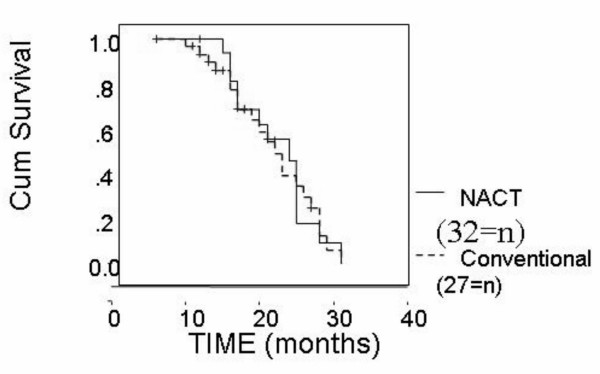
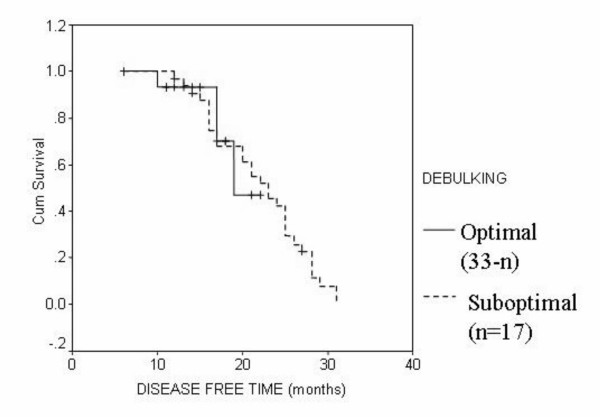
Results: Optimal cytoreduction was higher in the NACT group (72.2%) than the conventional group (62.4%), though not statistically significant (P = 0.5). More important was the finding that parameters of surgical aggressiveness (blood loss rates, ICU stay and total hospital stay) were significantly lower in NACT group than the conventional group. The median overall survival time was 28 months in the conventional group and 25 months in NACT group with a P value of 0.5. The median disease free survival was 19 months in the conventional group and 21 months in NACT group (P = 0.4). In multivariate analysis, the pathologic type and degree of debulking were found to affect the disease free survival significantly. Overall survival was not affected by any of the study parameters.
Conclusion: Primary chemotherapy followed by interval debulking surgery in select group of patients doesn't appear to worsen the prognosis, but it permits a less aggressive surgery to be performed.
Figures
References
-
- Frei E. Clinical cancer research, an embattled species. Cancer. 1982;50:1979–1992. - PubMed
LinkOut - more resources
Full Text Sources
