

Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial
- PMID: 16135917
- PMCID: PMC1357739
- DOI: 10.1097/01.sla.0000181092.50141.fa
Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial
Abstract
Objective: The objective of this study was to evaluate, in an international multicenter phase III trial, the accuracy, use, and morbidity of intraoperative lymphatic mapping and sentinel node biopsy (LM/SNB) for staging the regional nodal basin of patients with early-stage melanoma.
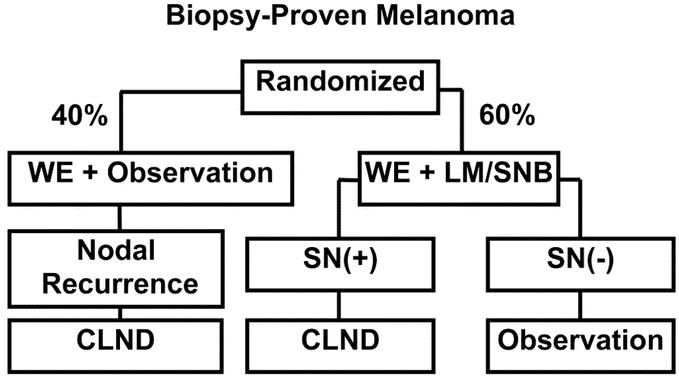
Summary background data: Since our introduction of LM/SNB in 1990, this technique has been widely adopted and has become part of the American Joint Committee on Cancer (AJCC) staging system. Eleven years ago, the authors began the international Multicenter Selective Lymphadenectomy Trial (MSLT-I) to compare 2 treatment approaches: wide excision (WE) plus LM/SNB with immediate complete lymphadenectomy (CLND) for sentinel node (SN) metastases, and WE plus postoperative observation with CLND delayed until the subsequent development of clinically evident nodal metastases.
Methods: After each center achieved 85% accuracy of SN identification during a 30-case learning phase, patients with primary cutaneous melanoma (> or =1 mm with Clark level > or =III, or any thickness with Clark level > or =IV) were randomly assigned in a 4:6 ratio to WE plus observation (WEO) with delayed CLND for nodal recurrence, or to WE plus LM/SNB with immediate CLND for SN metastasis. The accuracy of LM/SNB was determined by comparing the rates of SN identification and the incidence of SN metastases in the LM/SNB group versus the subsequent development of nodal metastases in the regional nodal basin of those patients with tumor-negative SNs. Early morbidity of LM/SNB was evaluated by comparing complication rates between the 2 treatment groups. Trial accrual was completed on March 31, 2002, after enrollment of 2001 patients.
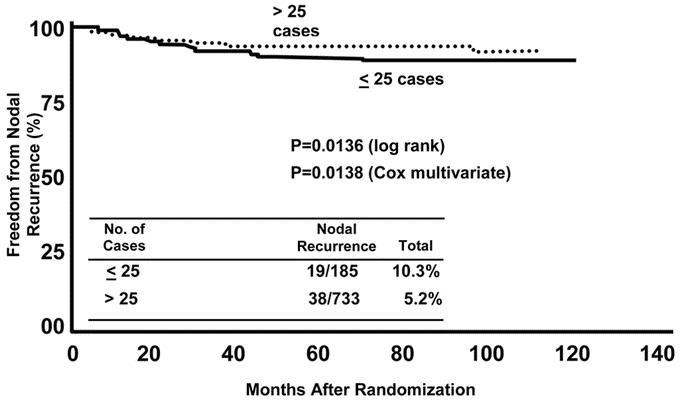
Results: Initial SN identification rate was 95.3% overall: 99.3% for the groin, 95.3% for the axilla, and 84.5% for the neck basins. The rate of false-negative LM/SNB during the trial phase, as measured by nodal recurrence in a tumor-negative dissected SN basin, decreased with increasing case volume at each center: 10.3% for the first 25 cases versus 5.2% after 25 cases. There were no operative mortalities. The low (10.1%) complication rate after LM/SNB increased to 37.2% with the addition of CLND; CLND also increased the severity of complications.
Conclusions: LM/SNB is a safe, low-morbidity procedure for staging the regional nodal basin in early melanoma. Even after a 30-case learning phase and 25 additional LM/SNB cases, the accuracy of LM/SNB continues to increase with a center's experience. LM/SNB should become standard care for staging the regional lymph nodes of patients with primary cutaneous melanoma.
Figures
Comment in
-
Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-1, an international multicenter trial.Ann Surg. 2007 Jan;245(1):156-7. doi: 10.1097/01.sla.0000250942.84678.8b. Ann Surg. 2007. PMID: 17197985 Free PMC article. No abstract available.
References
-
- Cochran AJ, Wen DR, Morton DL. Occult tumor cells in the lymph nodes of patients with pathological stage I malignant melanoma. An immunohistological study. Am J Surg Pathol. 1988;12:612–618. - PubMed
-
- Robinson DS, Sample WF, Fee HJ, et al. Regional lymphatic drainage in primary malignant melanoma of the trunk determined by colloidal gold scanning. Surg Forum. 1977;28:147–148. - PubMed
-
- Gaynor R, Irie R, Morton DL, et al. S100 protein is present in cultured human malignant melanomas. Nature. 1980;286:400–401. - PubMed
-
- Cochran AJ, Wen DR, Herschman HR. Occult melanoma in lymph nodes detected by antiserum to S-100 protein. Int J Cancer. 1984;34:159–163. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
