

Gabapentin for hot flashes in 420 women with breast cancer: a randomised double-blind placebo-controlled trial
- PMID: 16139656
- PMCID: PMC1627210
- DOI: 10.1016/S0140-6736(05)67215-7
Gabapentin for hot flashes in 420 women with breast cancer: a randomised double-blind placebo-controlled trial
Abstract
Background: Most women receiving systemic therapy for breast cancer experience hot flashes. We undertook a randomised, double-blind, placebo-controlled, multi-institutional trial to assess the efficacy of gabapentin in controlling hot flashes in women with breast cancer.
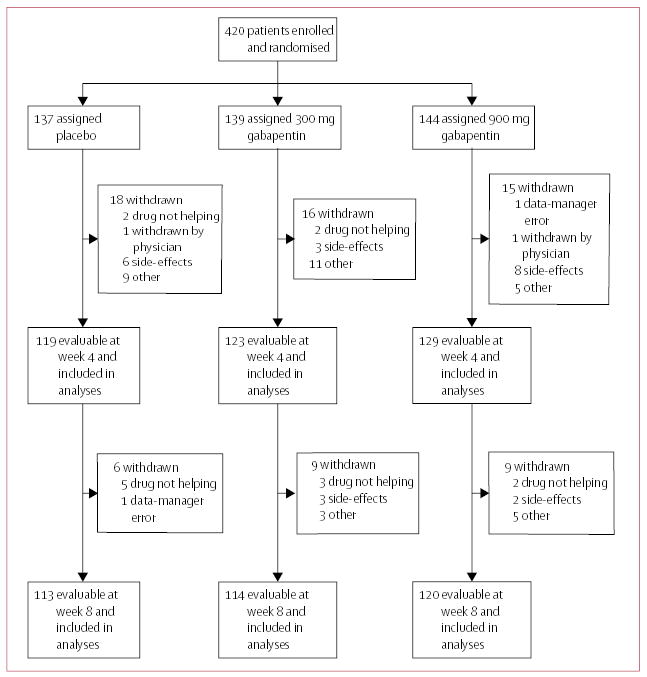
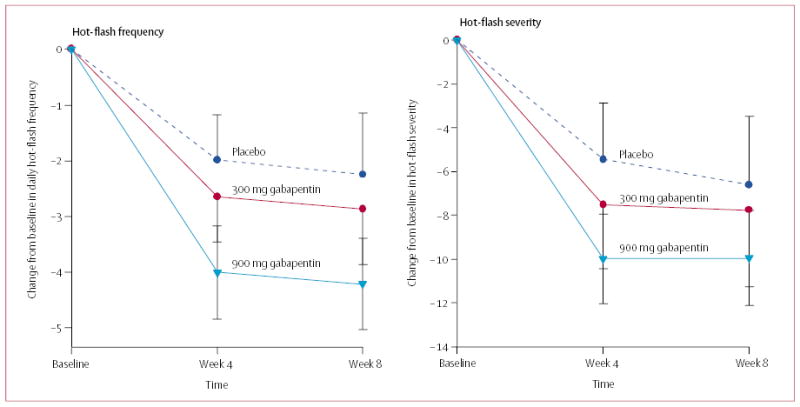
Methods: 420 women with breast cancer who were having two or more hot flashes per day were randomly assigned placebo, gabapentin 300 mg/day, or gabapentin 900 mg/day by mouth in three divided doses for 8 weeks. Each patient kept a 1-week, self-report diary on the frequency, severity, and duration of hot flashes before the start of the study and during weeks 4 and 8 of treatment. Analyses were by intention to treat.
Findings: Evaluable data were available on 371 participants at 4 weeks (119 placebo, 123 gabapentin 300 mg, and 129 gabapentin 900 mg) and 347 at 8 weeks (113 placebo, 114 gabapentin 300 mg, and 120 gabapentin 900 mg). The percentage decreases in hot-flash severity score between baseline and weeks 4 and 8, respectively were: 21% (95% CI 12 to 30) and 15% (1 to 29) in the placebo group; 33% (23 to 43) and 31% (16 to 46) in the group assigned gabapentin 300 mg; and 49% (42 to 56) and 46% (34 to 58) in the group assigned gabapentin 900 mg. The differences between the groups were significant (p=0.0001 at 4 weeks and p=0.007 at 8 weeks by ANCOVA for overall treatment effect, adjusted for baseline values); only the higher dose of gabapentin was associated with significant decreases in hot-flash frequency and severity.
Interpretation: Gabapentin is effective in the control of hot flashes at a dose of 900 mg/day, but not at a dose of 300 mg/day. This drug should be considered for treatment of hot flashes in women with breast cancer.
Figures
Comment in
-
900 mg daily of gabapentin was effective for hot flashes in women with breast cancer.ACP J Club. 2006 Mar-Apr;144(2):41. ACP J Club. 2006. PMID: 16539356 No abstract available.
References
-
- Carpenter JS, Andrykowski MA, Cordova M, et al. Hot flashes in postmenopausal women treated for breast carcinoma: prevalence, severity, correlates, management, and relation to quality of life. Cancer. 1998;82:1682–91. - PubMed
-
- Casper RF, Yen SS. Neuroendocrinology of menopausal flushes: an hypothesis of flush mechanism. Clin Endocrinol (Oxf ) 1985;22:293–312. - PubMed
-
- Freedman RR, Norton D, Woodward S, Cornelissen G. Core body temperature and circadian rhythm of hot flashes in menopausal women. J Clin Endocrinol Metab. 1995;80:2354–58. - PubMed
-
- Freedman RR, Krell W. Reduced thermoregulatory null zone in postmenopausal women with hot flashes. Am J Obstet Gynecol. 1999;181:66–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
