

Impediment in upper airway stabilizing forces assessed by phrenic nerve stimulation in sleep apnea patients
- PMID: 16146572
- PMCID: PMC1236961
- DOI: 10.1186/1465-9921-6-99
Impediment in upper airway stabilizing forces assessed by phrenic nerve stimulation in sleep apnea patients
Abstract
Background: The forces developed during inspiration play a key role in determining upper airway stability and the occurrence of nocturnal breathing disorders. Phrenic nerve stimulation applied during wakefulness is a unique tool to assess Upper airway dynamic properties and to measure the overall mechanical effects of the inspiratory process on UA stability.
Objectives: To compare the flow/pressure responses to inspiratory and expiratory twitches between sleep apnea subjects and normal subjects.
Methods: Inspiratory and expiratory twitches using magnetic nerve stimulation completed in eleven untreated sleep apnea subjects and ten normal subjects.
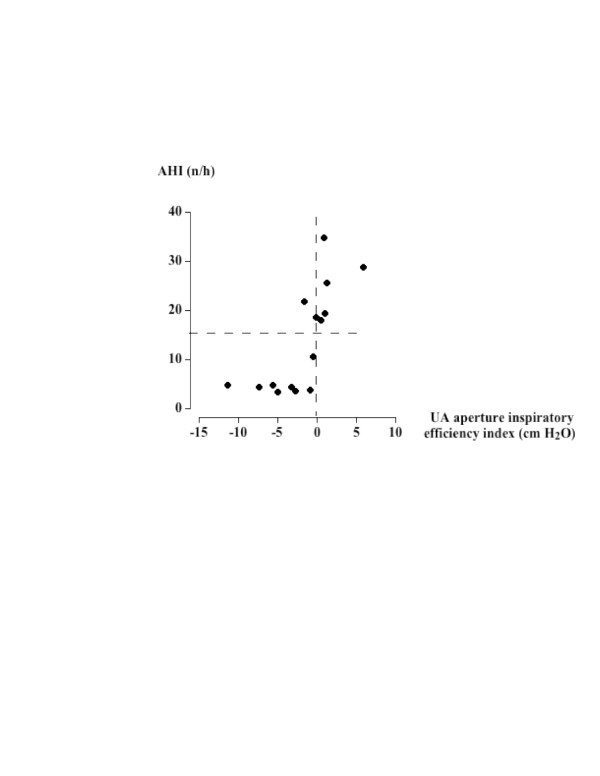
Results: In both groups, higher flow and pressure were reached during inspiratory twitches. The two groups showed no differences in expiratory twitch parameters. During inspiration, the pressure at which flow-limitation occurred was more negative in normals than in apneic subjects, but not reaching significance (p = 0.07). The relationship between pharyngeal pressure and flow adequately fitted with a polynomial regression model providing a measurement of upper airway critical pressure during twitch. This pressure significantly decreased in normals from expiratory to inspiratory twitches (-11.1 +/- 1.6 and -15.7 +/- 1.0 cm H2O respectively, 95% CI 1.6-7.6, p < 0.01), with no significant difference between the two measurements in apneic subjects. The inspiratory/expiratory difference in critical pressure was significantly correlated with the frequency of nocturnal breathing disorders.
Conclusion: Inspiratory-related upper airway dilating forces are impeded in sleep apnea patients.
Figures
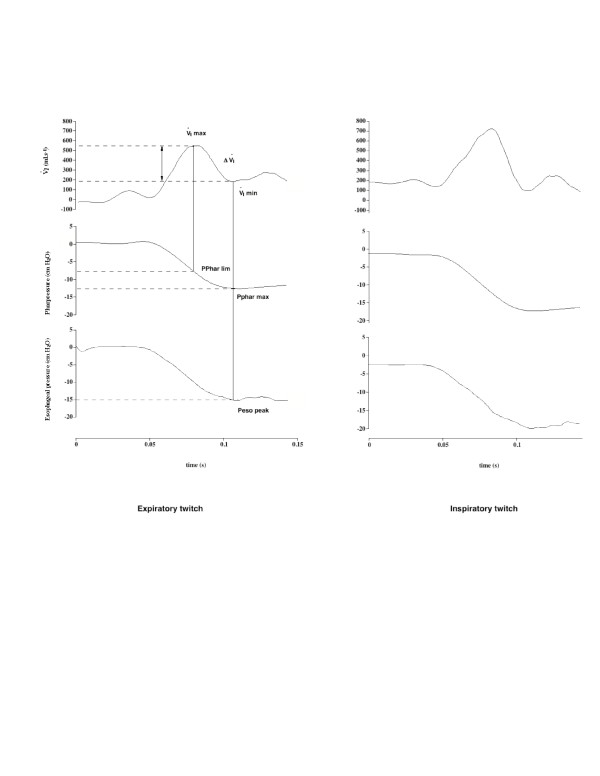
 I max and I min stand respectively for the maximal and minimal flow values reached during the twitch. Pphar lim indicates the pharyngeal pressure value corresponding to Imax. Peso peak indicates the driving pressure corresponding to I min. See text for abbreviations.
I max and I min stand respectively for the maximal and minimal flow values reached during the twitch. Pphar lim indicates the pharyngeal pressure value corresponding to Imax. Peso peak indicates the driving pressure corresponding to I min. See text for abbreviations.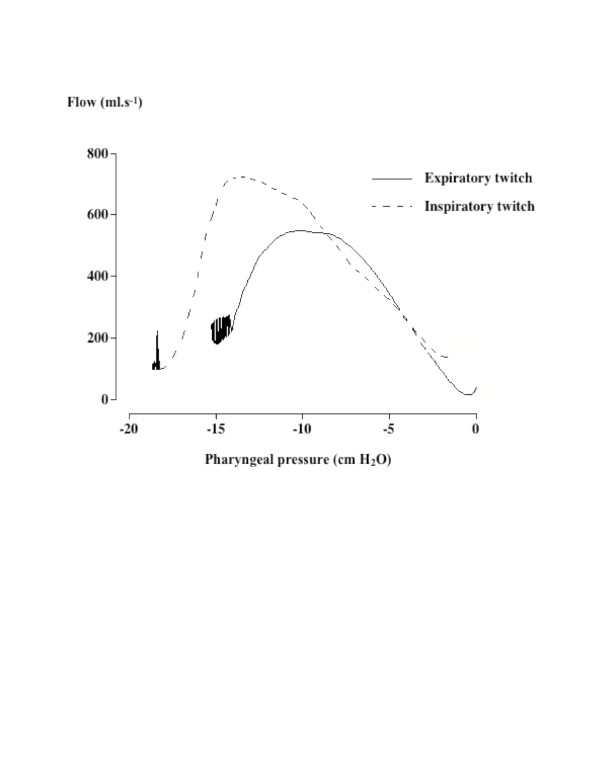 I max have been reached. A clear difference in the flow/pressure curves can be seen between the expiratory and inspiratory twitches.
I max have been reached. A clear difference in the flow/pressure curves can be seen between the expiratory and inspiratory twitches.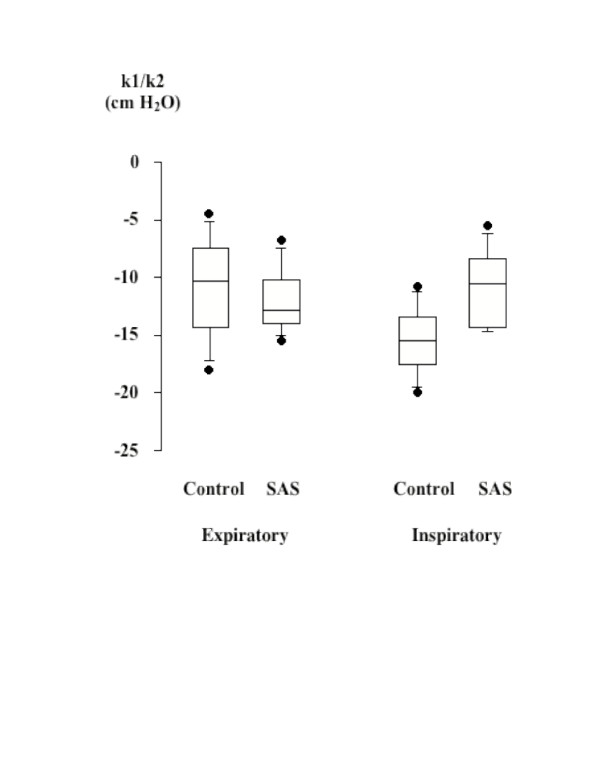
Similar articles
-
Inspiratory flow dynamics during phrenic nerve stimulation in awake normals during nasal breathing.Am J Respir Crit Care Med. 1999 Aug;160(2):614-20. doi: 10.1164/ajrccm.160.2.9812036. Am J Respir Crit Care Med. 1999. PMID: 10430737
-
Assessment of upper airway stabilizing forces with the use of phrenic nerve stimulation in conscious humans.J Appl Physiol (1985). 2003 Jun;94(6):2289-95. doi: 10.1152/japplphysiol.00924.2002. Epub 2003 Feb 21. J Appl Physiol (1985). 2003. PMID: 12598484
-
Assessment of upper airway dynamics in awake patients with sleep apnea using phrenic nerve stimulation.Am J Respir Crit Care Med. 2000 Sep;162(3 Pt 1):795-800. doi: 10.1164/ajrccm.162.3.9906135. Am J Respir Crit Care Med. 2000. PMID: 10988085
-
Pathophysiology of upper airway closure during sleep.JAMA. 1991 Sep 11;266(10):1384-9. JAMA. 1991. PMID: 1880868 Review.
-
Pathophysiology of upper airway obstruction during sleep.Clin Chest Med. 1998 Mar;19(1):21-32. doi: 10.1016/s0272-5231(05)70429-9. Clin Chest Med. 1998. PMID: 9554215 Review.
Cited by
-
Moderate-to-severe obstructive sleep apnea syndrome is associated with altered tongue motion during wakefulness.Eur Arch Otorhinolaryngol. 2023 May;280(5):2551-2560. doi: 10.1007/s00405-023-07854-9. Epub 2023 Jan 28. Eur Arch Otorhinolaryngol. 2023. PMID: 36707431
-
Anatomical feasibility of vagus nerve esophageal branch transfer to the phrenic nerve.Neural Regen Res. 2012 Mar 25;7(9):703-7. doi: 10.3969/j.issn.1673-5374.2012.09.011. Neural Regen Res. 2012. PMID: 25745467 Free PMC article.
-
Alteration of Swallowing and Ventilation Coordination in Respiratory Diseases in Small Mammals.Dysphagia. 2020 Apr;35(2):308-313. doi: 10.1007/s00455-019-10024-x. Epub 2019 Jun 21. Dysphagia. 2020. PMID: 31227886
-
Upper airway stabilization by osteopathic manipulation of the sphenopalatine ganglion versus sham manipulation in OSAS patients: a proof-of-concept, randomized, crossover, double-blind, controlled study.BMC Complement Altern Med. 2017 Dec 20;17(1):546. doi: 10.1186/s12906-017-2053-0. BMC Complement Altern Med. 2017. PMID: 29262824 Free PMC article. Clinical Trial.
References
-
- Guilleminault C, Van den Hoed J, Mitler M. Clinical overview of the sleep apnea syndrome. In: Guilleminault C, Dement WC, Alan R Liss, editor. Sleep apnea syndromes. New York; 1978. pp. 1–12.
-
- Shahar E, Whitney CW, Redline S, Lee T, Newman AB, Nieto J, O'Connor GT, Boland LL, Schwartz JE, Samet J. Sleep-disordered breathing and cardiovascular disease. Am J respir Crit Care Med. 2001;163:19–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
