

Risk assessment for biochemical recurrence prior to radical prostatectomy: significant enhancement contributed by human glandular kallikrein 2 (hK2) and free prostate specific antigen (PSA) in men with moderate PSA-elevation in serum
- PMID: 16152616
- PMCID: PMC1950472
- DOI: 10.1002/ijc.21474
Risk assessment for biochemical recurrence prior to radical prostatectomy: significant enhancement contributed by human glandular kallikrein 2 (hK2) and free prostate specific antigen (PSA) in men with moderate PSA-elevation in serum
Abstract
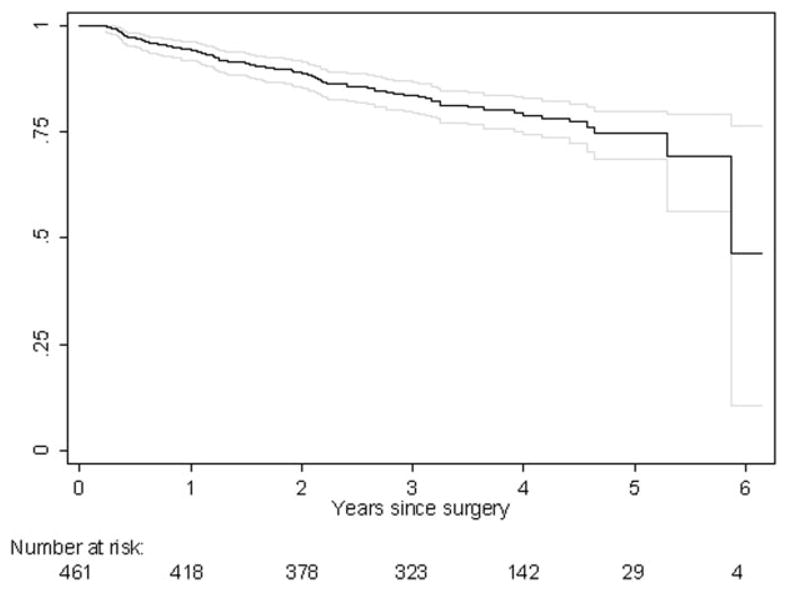
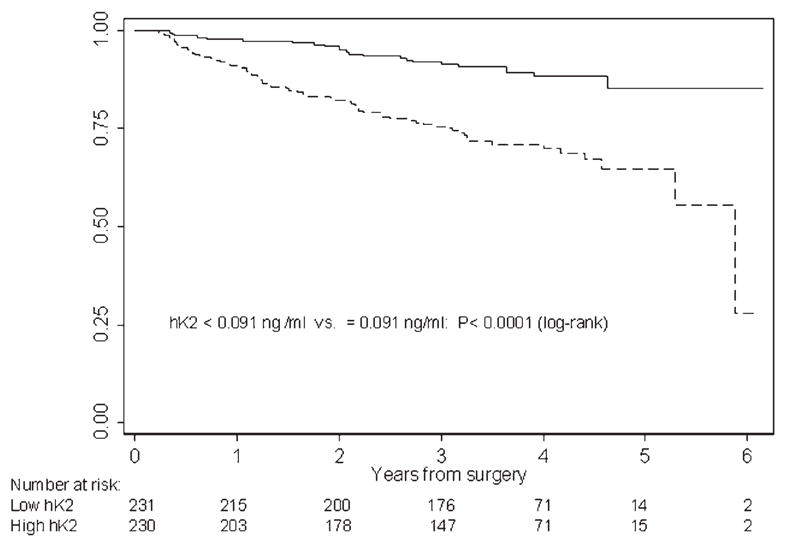
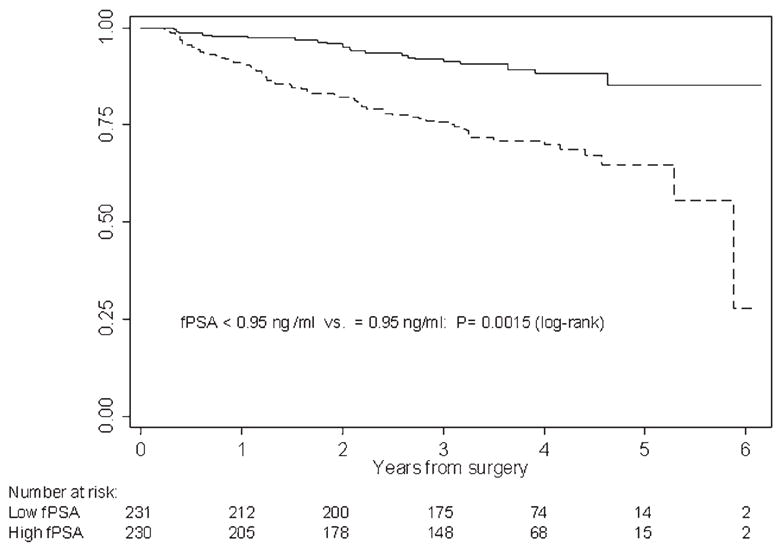
Most models to predict biochemical recurrence (BCR) of prostate cancer use pretreatment serum prostate-specific antigen (PSA), clinical stage and prostate biopsy Gleason grade. We investigated whether human glandular kallikrein 2 (hK2) and free prostate-specific antigen (fPSA) measured in pretreatment serum enhance prediction. We retrospectively measured total PSA (tPSA), fPSA and hK2 in preoperative serum samples from 461 men with localized prostate cancer treated with radical prostatectomy between 1999 and 2001. We developed a regression model to predict BCR using preoperative tPSA, clinical stage and biopsy Gleason grade. We then compared the predictive accuracy of this "base" model with a model with fPSA and hK2 as additional predictors. BCR was observed in 90 patients (20%), including 48 patients with a pretreatment tPSA < or = 14 ng/ml (13%), and 28 patients (10%) with a pretreatment tPSA < or = 10 ng/ml. Overall, the predictive accuracy of the base model (bootstrap-corrected concordance index of 0.813) was not improved after the addition of fPSA or hK2 (0.818). However, for men with moderate tPSA-elevation (tPSA < or = 10 ng/ml), addition of fPSA and hK2 data increased predictive accuracy (from a base model concordance index of 0.756-0.815, p = 0.005). The improvement in accuracy was not sensitive to the threshold for "moderately elevated" PSA. For patients with a moderate tPSA-elevation (tPSA < or = 10 ng/ml), which closely corresponds to concurrent disease demographics, BCR-prediction was enhanced when fPSA and hK2 were added to the conventional model. Measurements of fPSA and hK2 improve on our ability to counsel patients prior to treatment as to their risk of BCR.
(c) 2005 Wiley-Liss, Inc.
Conflict of interest statement
In full disclosure of potential conflicts of interest, we would like to notify you that Dr. Hans Lilja is a patent holder of the free PSA and hK2 Immunoassay. The authors further confirm that no further relationship exists that could be construed as resulting in an actual, potential or apparent conflict of interest with the manuscript submitted for review.
Figures
References
-
- Hull GW, Rabbani F, Abbas F, Wheeler TM, Kattan MW, Scardino PT. Cancer control with radical prostatectomy alone in 1,000 consecutive patients. J Urol. 2002;167:528–34. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–7. - PubMed
-
- Gerber GS, Thisted RA, Scardino PT, Frohmuller HG, Schroeder FH, Paulson DF, Middleton AW, Jr, Rukstalis DB, Smith JA, Jr, Schell-hammer PF, Ohori M, Chodak GW. Results of radical prostatectomy in men with clinically localized prostate cancer. JAMA. 1996;276:615–9. - PubMed
-
- D’Amico AV, Whittington R, Malkowicz SB, Fondurulia J, Chen MH, Kaplan I, Beard CJ, Tomaszewski JE, Renshaw AA, Wein A, Coleman CN. Pretreatment nomogram for prostate-specific antigen recurrence after radical prostatectomy or external-beam radiation therapy for clinically localized prostate cancer. J Clin Oncol. 1999;17:168–72. - PubMed
-
- Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst. 1998;90:766–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
