

Aggregate analysis of the literature for unruptured intracranial aneurysm treatment
- PMID: 16155132
- PMCID: PMC8148866
Aggregate analysis of the literature for unruptured intracranial aneurysm treatment
Abstract
Background: Publication bias and/or true heterogeneity can skew aggregate impressions from scientific literature. To better determine aggregate measures for unruptured intracranial aneurysm (UIA) treatment, we analyzed adverse outcome rates of surgical clipping and endovascular coil embolization.
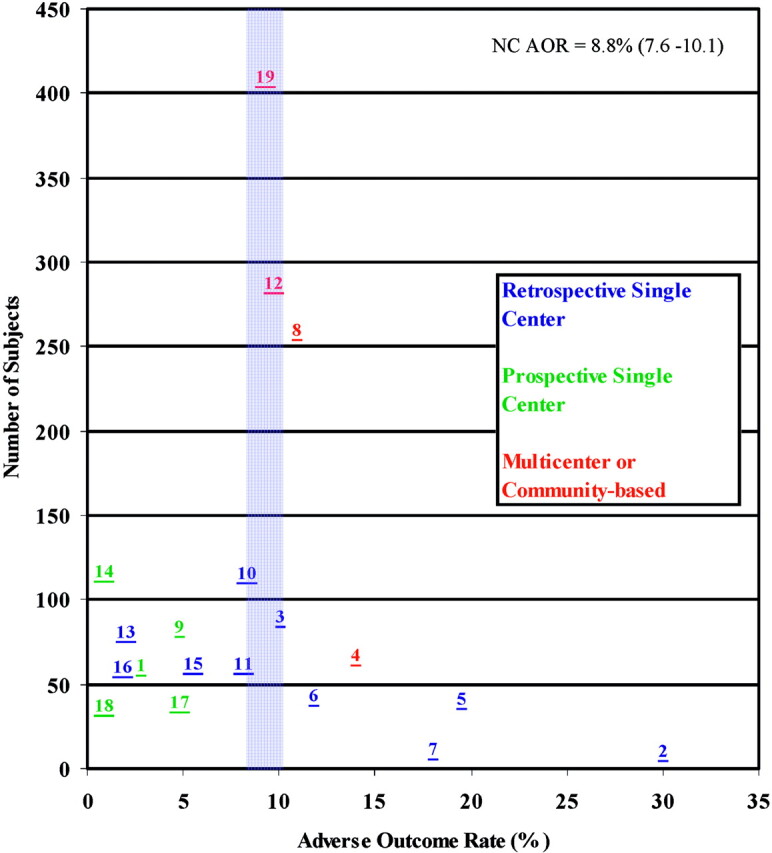
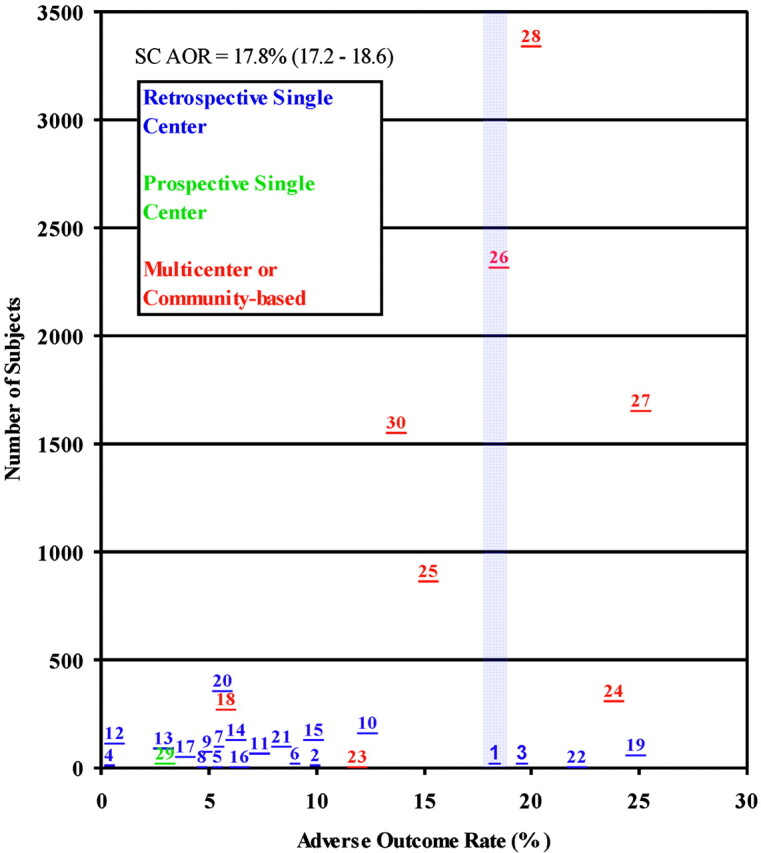
Methods: Two independent reviewers searched MEDLINE for studies publishing adverse outcome rates for endovascular coiling and surgical clipping between January 1990 and July 2003. Studies were classified as single-center, multicenter, or community-based. We defined adverse outcome rates as combined all-cause early or in-hospital morbidity and mortality. We determined cumulative adverse outcome rates by plotting precision measure (sample size) against trial-specific effect (adverse outcome rate).
Findings: We included 4 endovascular coiling multicenter/community-based studies (1019 patients) and 13 single-center studies (810 patients) and 5 surgical clipping multicenter/community-based studies (10,541 patients) and 23 single-center studies (1759 patients). Cumulative adverse outcome rates for endovascular coiling and surgical clipping were 8.8% (95% confidence interval [CI] 7.6%-10.1%) and 17.8% (95% CI 17.2%-18.6%).
Interpretation: Scattergram distribution illustrated the magnitude of bias in current literature reporting UIAs. Major parts of the literature may have underestimated surgical clipping morbidity and mortality, which can be attributed to bias from smaller retrospective studies. Neuroradiologic coiling studies were less likely to include factors contributing to inaccurate adverse outcome rates.
Figures
References
-
- Light R, Pillemer DB. Summing up: the science of reviewing research. Cambridge, MA: Harvard University Press;1984
-
- Johnston SC, Zhao S, Dudley RA, et al. Treatment of unruptured cerebral aneurysms in California. Stroke 2001;32:597–605 - PubMed
-
- Wiebers DO, Whisnant JP, Huston J 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003;362:103–110 - PubMed
-
- Eskridge JM, Song JK. Endovascular embolization of 150 basilar tip aneurysms with Guglielmi detachable coils: results of the Food and Drug Administration multicenter clinical trial. J Neurosurg 1998;89:81–86 - PubMed
-
- Bavinzski G, Killer M, Gruber A, et al. Treatment of basilar artery bifurcation aneurysms by using Guglielmi detachable coils: a 6-year experience. J Neurosurg 1999;90:843–852 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical