

Radiation necrosis versus glioma recurrence: conventional MR imaging clues to diagnosis
- PMID: 16155144
- PMCID: PMC8148818
Radiation necrosis versus glioma recurrence: conventional MR imaging clues to diagnosis
Abstract
Background and purpose: Conventional MR imaging findings are considered to be inadequate for reliably distinguishing radiation necrosis from tumor recurrence in patients with glioma. Despite this belief, we hypothesized that certain conventional MR imaging findings, alone or in combination, though not definitive, may favor one or another of these diagnoses in proton beam-treated patients with new enhancing lesions on serial scanning.
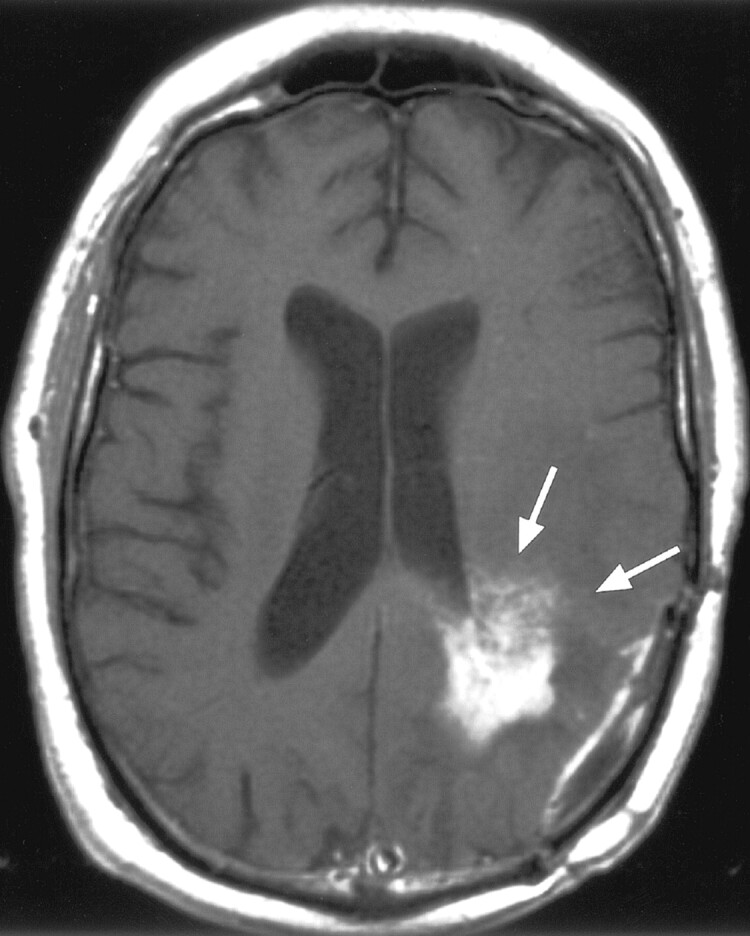
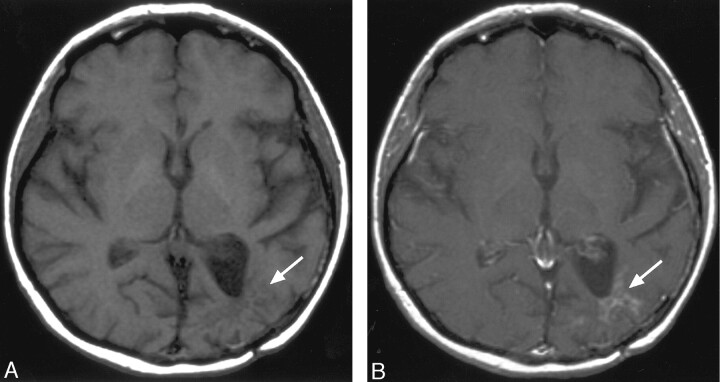
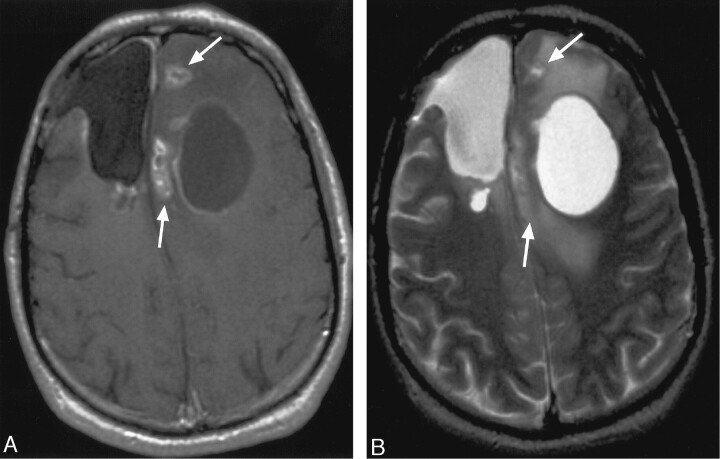
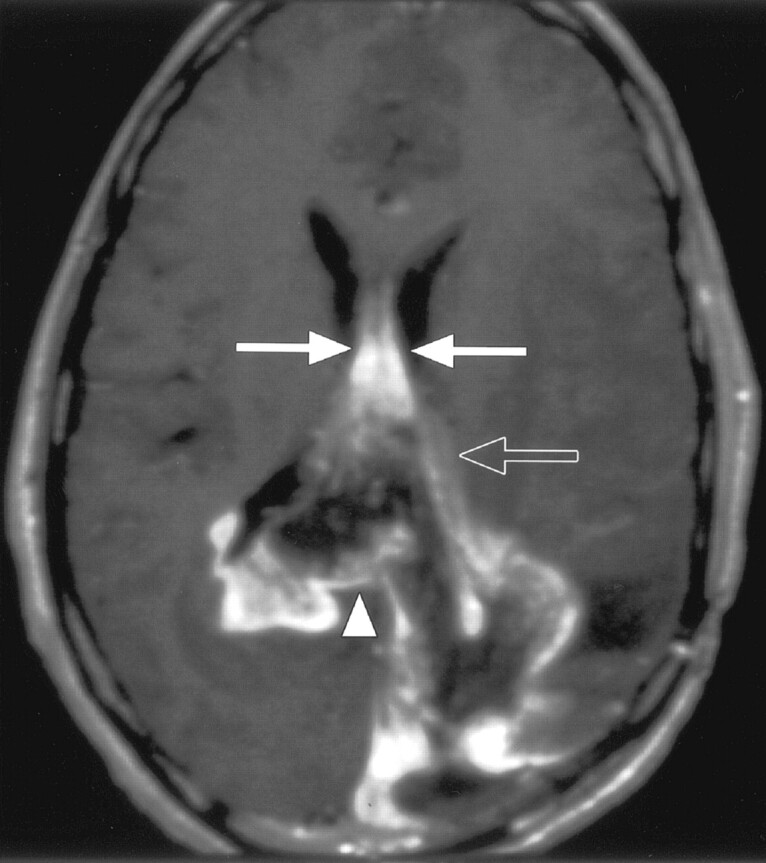
Methods: MR imaging findings (axial T1-, T2-, and post-gadolinium T1-weighted) of 27 proton beam radiation therapy patients with high-grade gliomas were retrospectively reviewed. Entry criteria included new MR imaging enhancing lesions after treatment and histologically unequivocal biopsy proof of diagnosis. Readers rated corpus callosum involvement, midline spread, subependymal spread, new discrete multiple enhancing foci, a "spreading wavefront" appearance, and septum pellucidum involvement. Statistical analysis was by the Fisher exact test.
Results: Corpus callosum involvement in combination with multiple other findings was highly associated with progressive glioma. These combinations included involvement of the corpus callosum with multiple enhancing foci (P = .02), involvement of the corpus callosum with crossing the midline and multiple enhancing lesions (P = .04), and involvement of the corpus callosum with subependymal spread and multiple enhancing lesions (P = .01).
Conclusions: In proton beam-treated patients with glioma, corpus callosum involvement, in conjunction with multiple enhancing lesions with or without crossing of the midline and subependymal spread, favors predominant glioma progression. Overall, combinations of enhancement patterns were more likely than individual patterns to distinguish necrosis from predominant tumor progression. Together with clinical and functional imaging findings, these results may assist in determining the need for biopsy.
Figures
References
-
- Chan YL, Yeung DK, Leung SF, Chan PN. Diffusion-weighted magnetic resonance imaging in radiation-induced cerebral necrosis: apparent diffusion coefficient in lesion components. J Comput Assist Tomogr 2003;27:674–680 - PubMed
-
- Aksoy FG, Lev MH. Dynamic contrast-enhanced brain perfusion imaging: technique and clinical applications. Semin Ultrasound CT MR 2000;21:462–477 - PubMed
-
- Aronen HJ, Perkio J. Dynamic susceptibility contrast MRI of gliomas. Neuroimaging Clin N Am 2002;12:501–523 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical