

West Nile virus meningoencephalitis: MR imaging findings
- PMID: 16155147
- PMCID: PMC8148846
West Nile virus meningoencephalitis: MR imaging findings
Abstract
Background and purpose: Reports of MR imaging in West Nile virus (WNV) meningoencephalomyelitis are few and the described findings limited. The purpose of this study was to review the spectrum of MR imaging findings for WNV meningoencephalomyelitis and investigate whether any of the findings correlates with clinical presentation of flaccid paralysis.
Methods: We reviewed the MR imaging findings of 17 patients with confirmed WNV encephalitis and/or myelitis. MR imaging brain studies were evaluated for location of signal intensity abnormalities, edema, hydrocephalus, or abnormal enhancement. MR imaging spine studies were evaluated for signal intensity abnormalities in cord and/or enhancement.
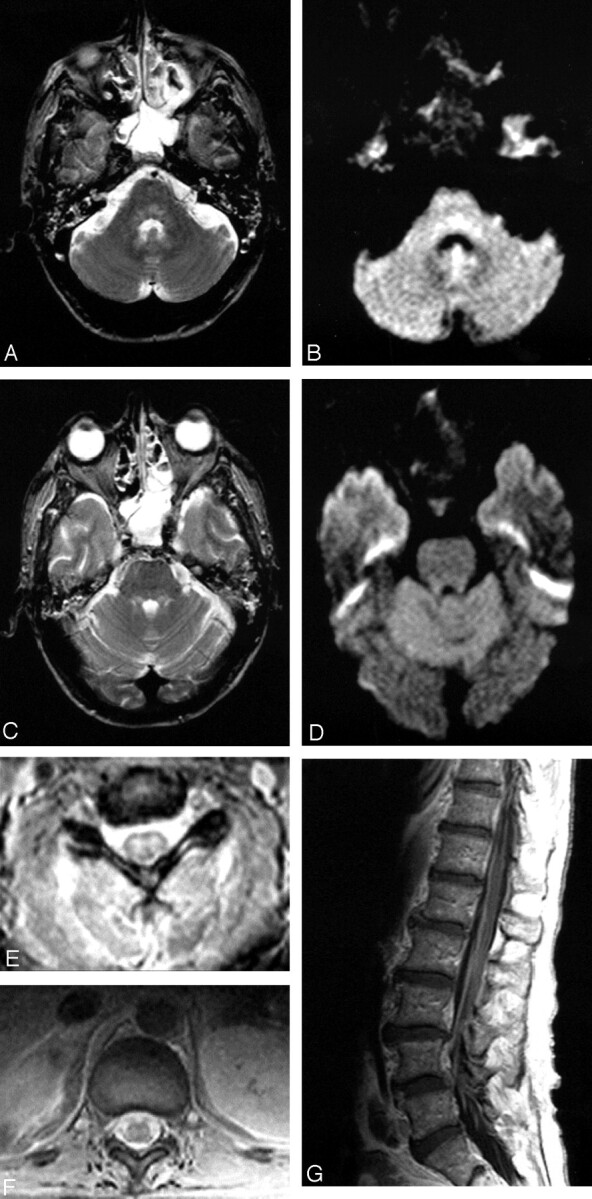
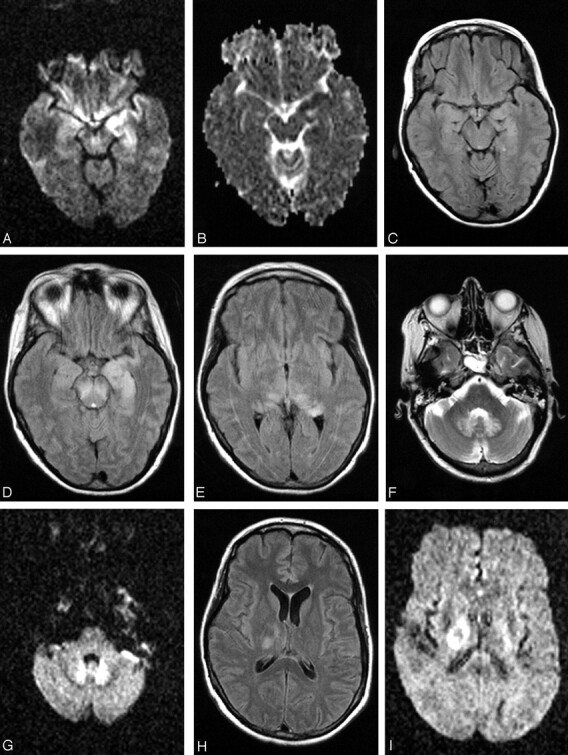
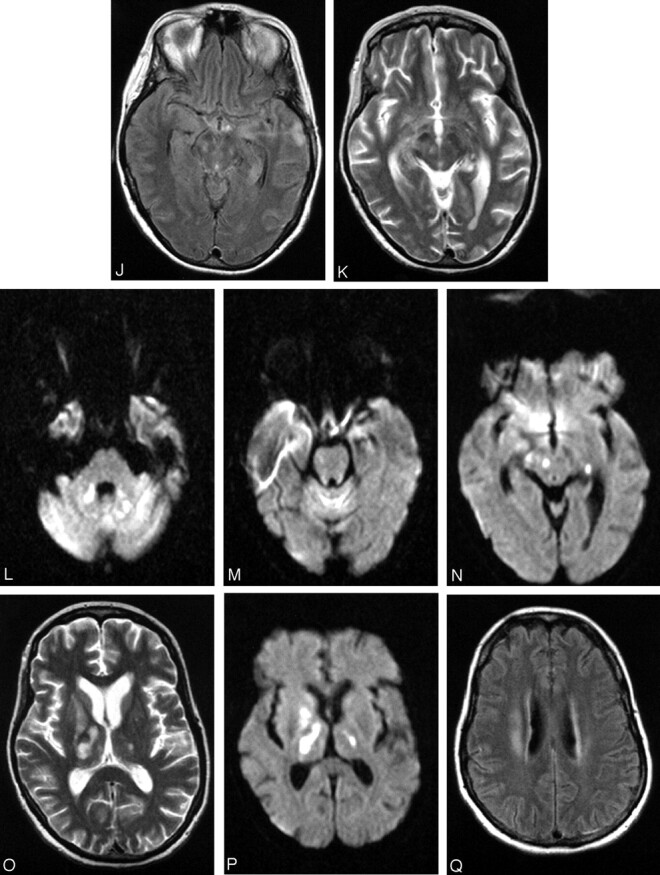
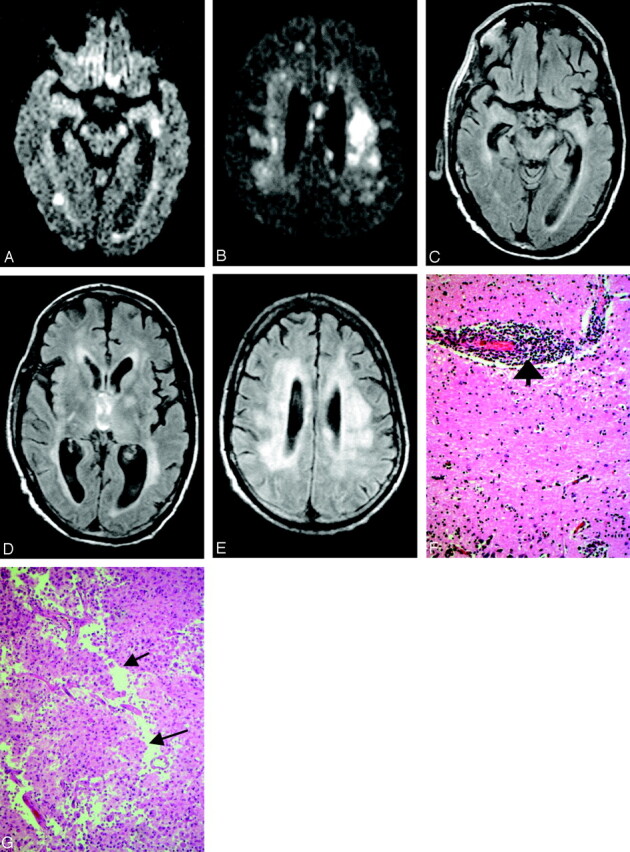
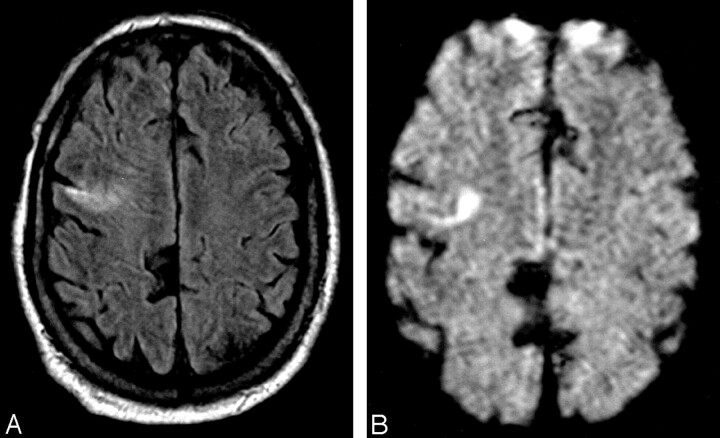
Results: Retrospective review of the MR imaging studies of 17 patients was performed by 2 neuroradiologists. Eleven of 16 brain MR images demonstrated abnormalities. Eight (50%) patients had abnormal studies related to meningoencephalitis. All 8 patients had abnormal findings in the deep gray matter and/or brain stem; 2 had additional white matter abnormalities. Three patients with abnormal MR studies of the spine had extremity weakness on examination. The imaging findings included abnormal signal intensity more pronounced in the ventral horns and/or enhancement around the conus medullaris and cauda equina. One patient had additional abnormalities in the pons.
Conclusion: Abnormal MR imaging findings in patients with WNV meningoencephalomyelitis are nonspecific but not uncommon. Anatomic areas commonly affected are basal ganglia, thalami, mesial temporal structures, brain stem, and cerebellum. Extremity weakness or flaccid paralysis corresponds to spinal cord/cauda equina abnormalities.
Figures

References
-
- Nash D, Mostashari F, Fine A, et al. The outbreak of West Nile virus infection in New York City area in 1999. N Engl J Med 2001;344:1807–1814 - PubMed
-
- Jeha LE, Sila CA, Lederman RJ, et al. West Nile virus infection: a new acute paralytic illness. Neurology 2003;61:55–59 - PubMed
-
- Olsan A, Milburn JM, Baumgarten KL, Durham HL. Leptomeningeal enhancement in a patient with proven West Nile virus infection. AJR Am J Roentgenol 2003;181:591–592 - PubMed
-
- Lanciotti RS, Roehrig JT, Deubel V, et al. Origin of the West Nile virus responsible for an outbreak of encephalitis in the northeastern United States. Science 1999;286:2333–2337 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical