

Imaging manifestations of spinal fractures in ankylosing spondylitis
- PMID: 16155161
- PMCID: PMC8148850
Imaging manifestations of spinal fractures in ankylosing spondylitis
Abstract
Background and purpose: Spinal fractures in ankylosing spondylitis (AS) were difficult to diagnose before CT and MR imaging were available. The purpose of our investigation was to characterize spinal fractures and determine the value of different imaging modalities in AS.
Methods: Twelve successive cases of spinal fractures were identified in MR imaging files of AS patients. Conventional radiographs were available for 12, CT scans for 7, and 3D-CT scans for 4. We carefully reviewed clinical histories and imaging presentations.
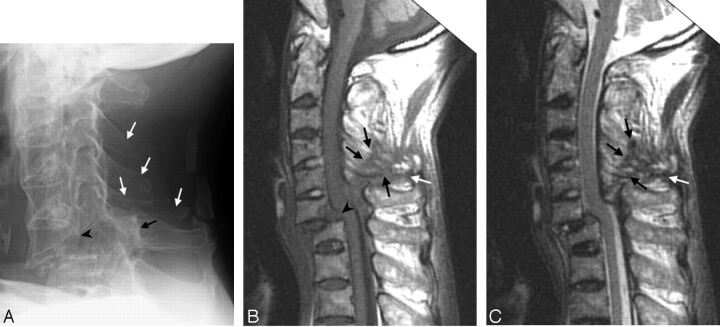
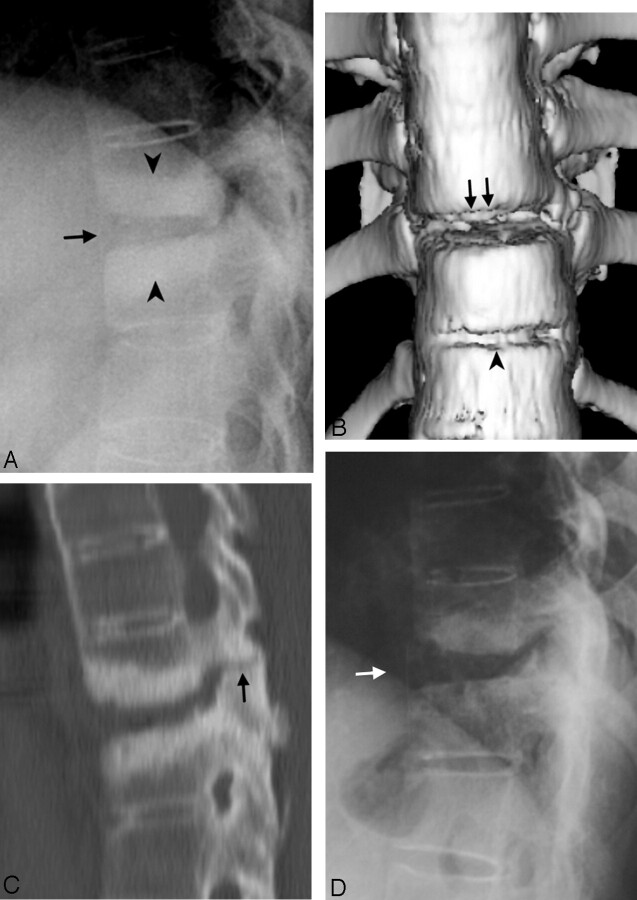
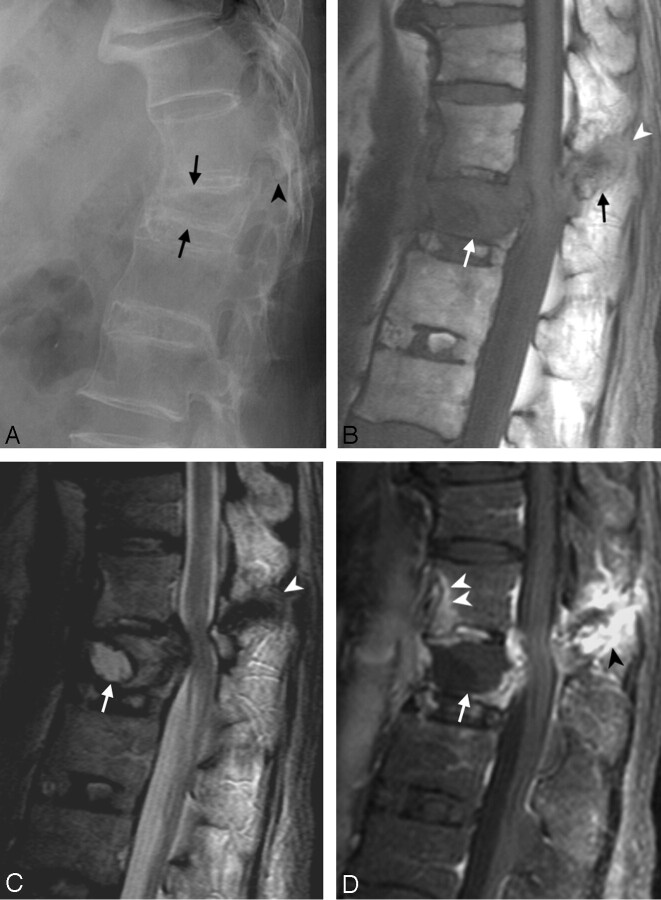
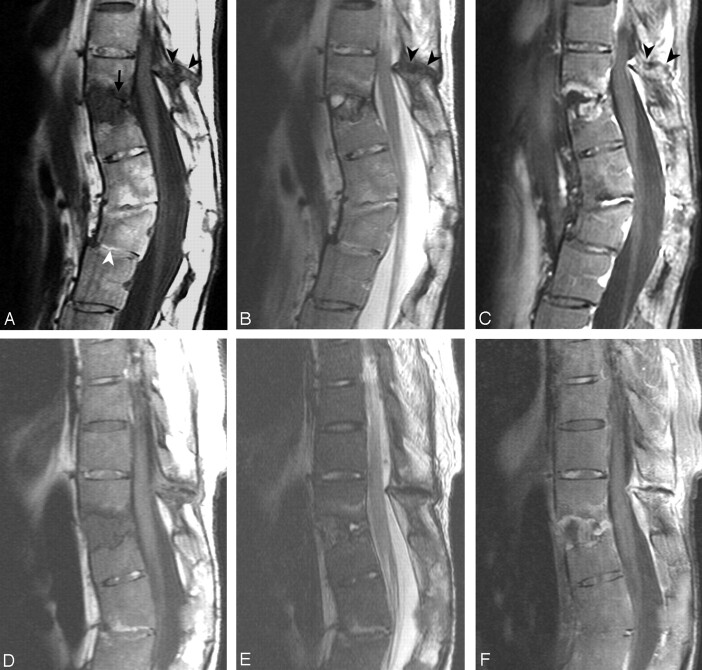
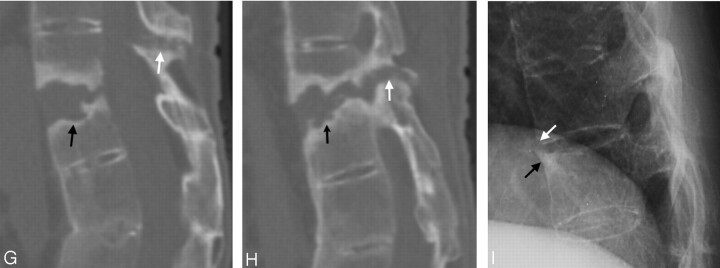
Results: Fractures were found in the cervical spine in 3 patients and in the thoracolumbar spine in 9. The 3 columns of the spine were involved in 11 patients. A routine 4-mm axial CT was not enough to demonstrate all fractures and ligament tears. The sensitivities of 3D-CT scans for demonstration of the following problems were similar to that of MR imaging and were better than that of conventional radiographs: tearing of the posterior longitudinal ligament, the thoracic spinous process fracture, and the facet fracture. MR imaging depicted these following findings that usually were not shown on conventional radiographs or 3D-CT scans: cord deformity, soft tissue disruption, and ligament tears in the posterior column. MR imaging also showed avascular necrosis and occult fractures better than conventional radiographs or CT scans.
Conclusions: MR imaging shows abnormalities in AS that may not be clear or even detectable by using other imaging methods. With the capability to show lesions in the posterior column, MR imaging can serve to evaluate AS patients with spinal fracture for the possibility of 3-column involvement.
Figures
References
-
- Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord 1999;37:444–447 - PubMed
-
- Lawrence JS. The prevalence of arthritis. Br J Clin Pract 1963;17:699. - PubMed
-
- Hitchon PW, From AM, Brenton MD, et al. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg 2002;97(2 suppl):218–222 - PubMed
-
- Graham GP, Evans PD. Spinal fractures in patients with ankylosing spondylitis. Injury 1991;22:426–427 - PubMed
-
- Gartman JJ Jr, Bullitt E, Baker ML. Axis fracture in ankylosing spondylitis: case report. Neurosurgery 1991;29:590–593 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials