

Identification, prognosis, and management of patients with carotid artery near occlusion
- PMID: 16155163
- PMCID: PMC8148868
Identification, prognosis, and management of patients with carotid artery near occlusion
Abstract
Background and purpose: Two large trials indicated that endarterectomy was less beneficial for symptomatic patients with internal carotid artery (ICA) near occlusion than for patients who had severe stenosis without near occlusion. Near occlusions complicate ratio calculations of ICA stenosis and require attention to detail for identification. The goal is to provide diagnostic criteria, illustrate identifying features, estimate accuracy of identification, and assess prognosis for patients with near occlusion.
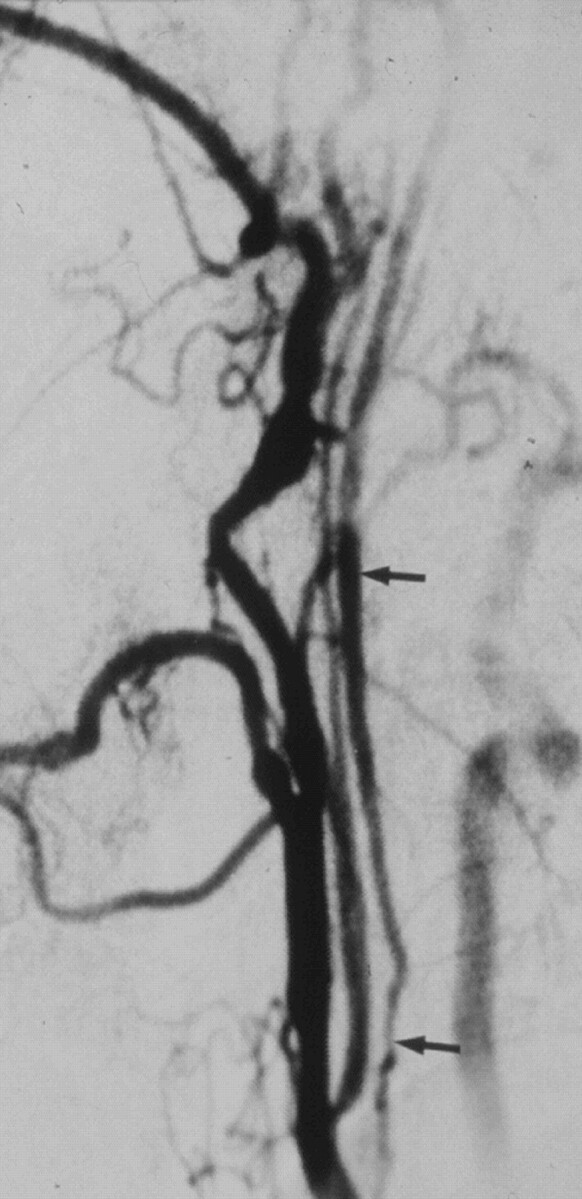
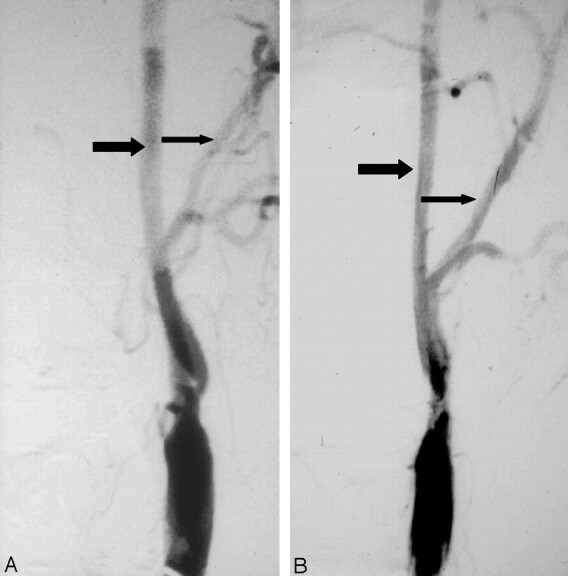
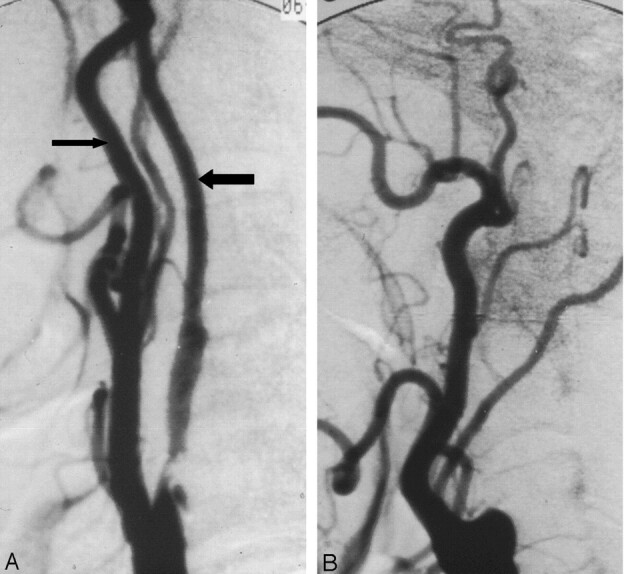
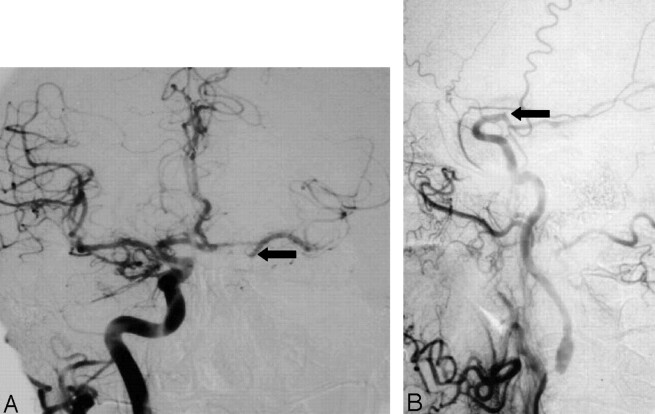
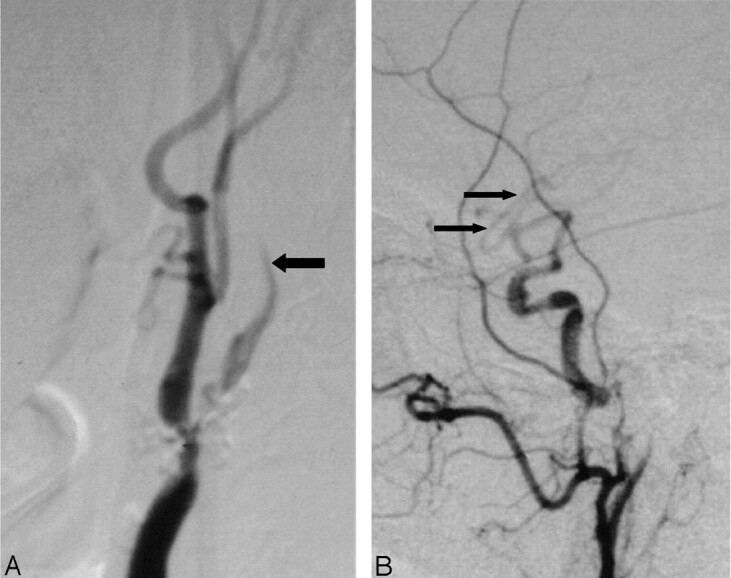
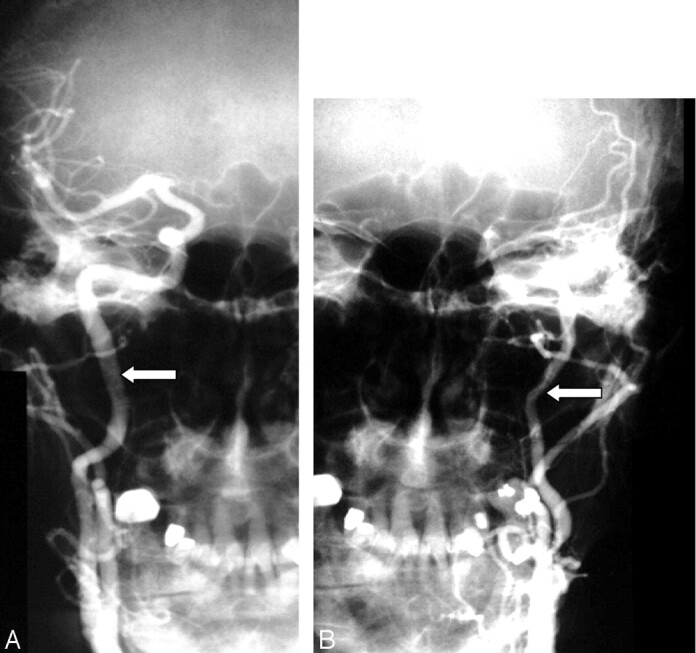
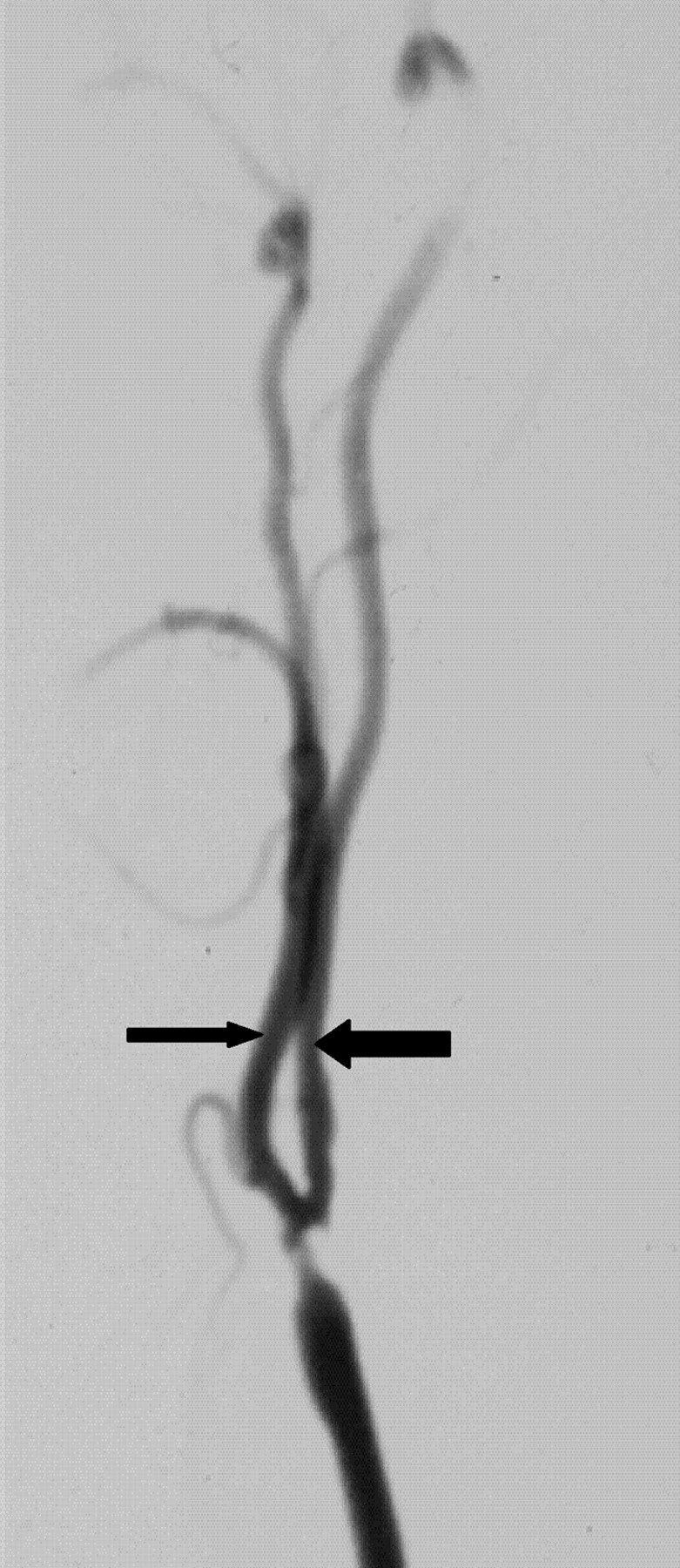
Methods: We re-reviewed 1216 patients with severe (> or =70%) stenosis on angiography in the North American Symptomatic Carotid Endarterectomy Trial and European Carotid Surgery Trial. One of 5 (n = 262) had 2 or more criteria for near occlusion: (1) delayed cranial arrival of ICA contrast compared with external carotid artery (ECA); (2) intracranial collaterals seen as cross-filling of contralateral vessels or ipsilateral contrast dilution; (3) obvious diameter reduction of ICA compared with opposite ICA; or (4) ICA diameter reduction compared with ipsilateral ECA.
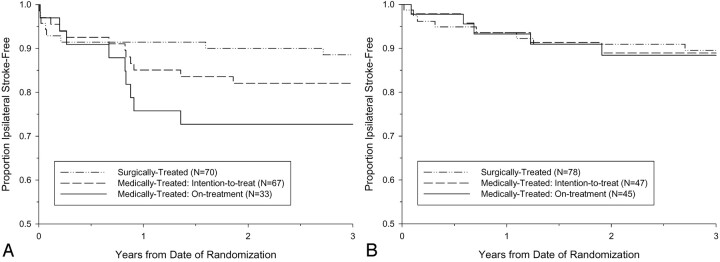
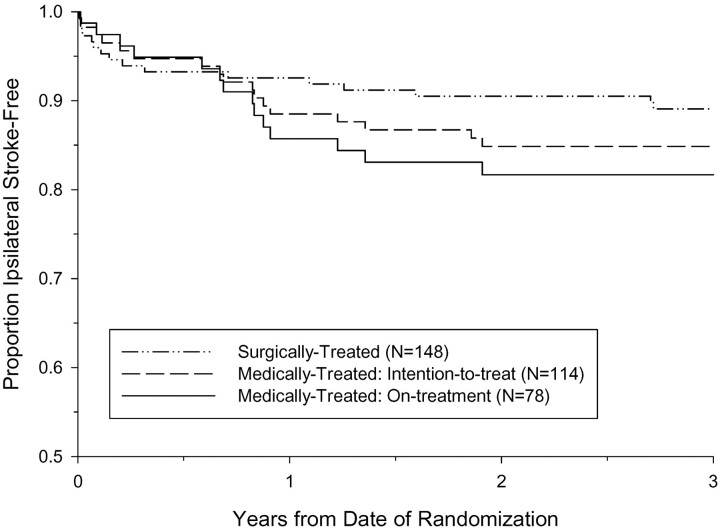
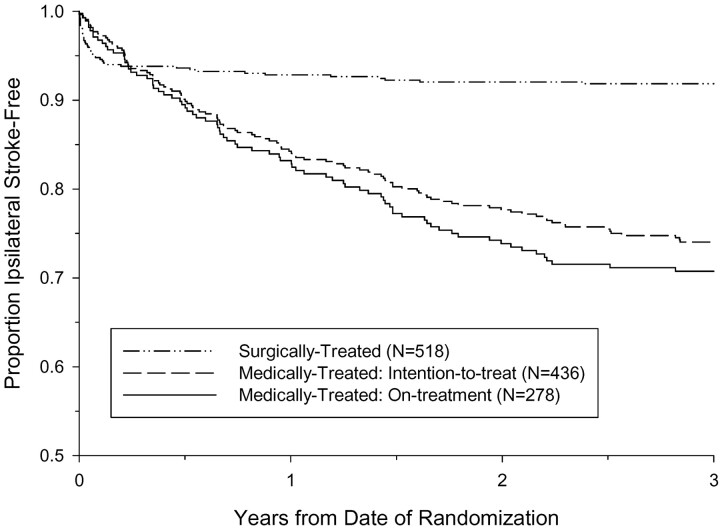
Results: Interrater agreement, sensitivity, and specificity were excellent (0.88, 90.6%, and 93.8%, respectively). By intention to treat, 3-year risks of ipsilateral stroke for medically treated patients with near occlusion was 15.1% versus 10.9% for surgically treated (absolute risk reduction [ARR] = 4.2%; P value = .33). Patients who continued to receive treatment in the medical arm for the trial's duration had a 3-year risk of 18.3% (ARR = 7.4%; P value = .13). Medically treated patients with severe stenosis but without near occlusion had a 3-year risk of 26.0% versus surgically treated of 8.2% (ARR = 17.8%; P value < .001).
Conclusion: It is crucial to identify near occlusions on vascular imaging. Although it still is reasonable to consider endarterectomy for these patients, the benefit is muted.
Figures
References
-
- Berman SS, Devine JJ, Erodes LS, Hunter GC. Distinguishing carotid artery pseudo-occlusion with color flow Doppler. Stroke 1995;26:434–438 - PubMed
-
- Fox AJ. How to measure carotid stenosis. Radiology 1993;186:316–318 - PubMed
-
- Gabrielsen TO, Seeger JF, Knake JE, et al. The nearly occluded internal carotid artery: a diagnostic trap. Radiology 1981;138:611–618 - PubMed
-
- Henderson R, Eliasziw M, Fox AJ, et al. The importance of angiographically defined collateral circulation in patients with severe carotid stenosis. Stroke 2000;31:128–132 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous