

Review
doi: 10.1136/hrt.2004.046334.
Genetics of cardiac arrhythmias
Affiliations
- PMID: 16162633
- PMCID: PMC1769155
- DOI: 10.1136/hrt.2004.046334
Item in Clipboard
Review
Genetics of cardiac arrhythmias
Heart.
2005 Oct.
No abstract available
Figures
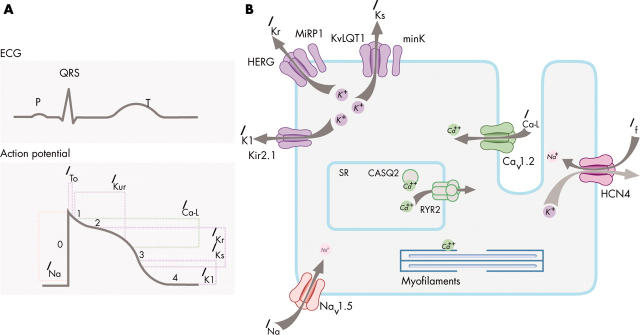
Ionic currents contributing to the ventricular action potential (A) and schematic representation of a cardiomyocyte displaying (only) those proteins involved in the pathogenesis of inherited arrhythmia syndromes (B). In panel A, the action potential is aligned with its approximate time of action during the ECG. In panel B, ankyrin-B, an adapter protein involved in the long QT syndrome type 4, is not depicted.
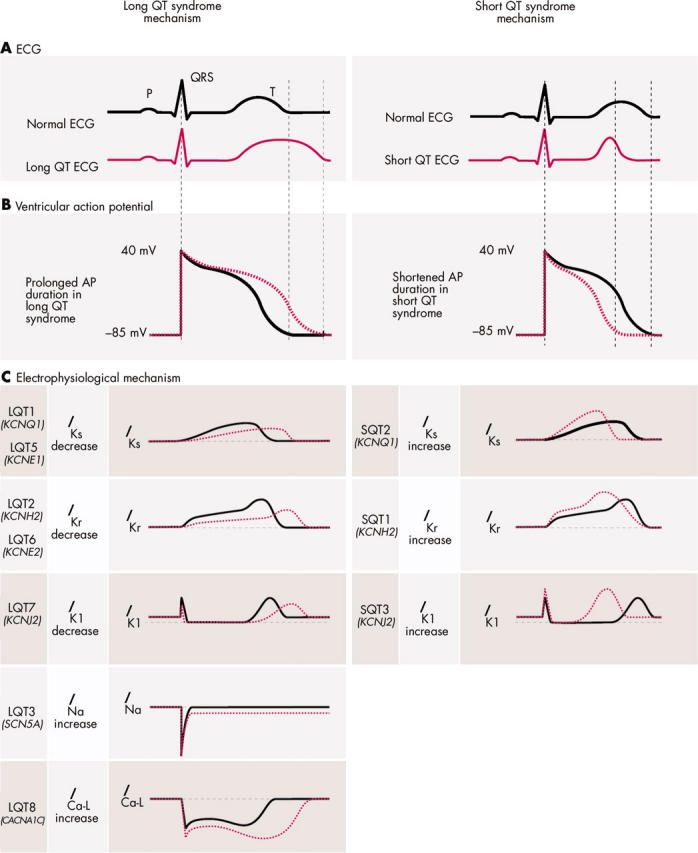
Pathophysiologic mechanisms of ion channel mutations in long QT syndrome (LQTS) and short QT syndrome (SQTS). (A) Schematic ECG representation. The red dotted line represents QT interval prolongation (left panel) and shortening (right panel) as can be observed in the LQTS and SQTS, respectively. (B) The ventricular action potential (AP). The red dotted line represents prolongation (left) and shortening (right) of action potential duration (APD) as can be observed in the LQTS and SQTS, respectively. (C) Effect of mutations on current characteristics in LQTS (left) and SQTS (right). By convention, upward (positive) deflections represent outward current, downward (negative) deflections represent inward current. Normal (solid grey line) and abnormal (dotted red line) current characteristics are aligned with their approximate time of action during the ECG (A) and the ventricular AP (B). A reduced IKs activity underlies APD prolongation in LQT1 and 5, while an increased IKs activity underlies APD shortening in SQT2. A reduced IKr activity underlies APD prolongation in LQT2 and 6, while an increased IKr activity underlies APD shortening in SQT1. A reduced IK1 activity during the terminal phase of repolarisation underlies APD prolongation in LQT7, while an increased IK1 activity underlies APD shortening in SQT3. An enhanced INa and an enhanced ICa-L during the AP plateau prolong APD in LQT3 and LQT8, respectively.
References
-
- Roden DM, Balser JR, George AL Jr, et al. Cardiac ion channels. Annu Rev Physiol 2002;64:431–75. - PubMed
-
- Clancy CE, Kass RS. Inherited and acquired vulnerability to ventricular arrhythmias: cardiac Na+ and K+ channels. Physiol Rev 2005;85:33–47. - PubMed
-
- Mohler PJ, Schott JJ, Gramolini AO, et al. Ankyrin-B mutation causes type 4 long-QT cardiac arrhythmia and sudden cardiac death. Nature 2003;421:634–9. - PubMed
-
- Plaster NM, Tawil R, Tristani-Firouzi M, et al. Mutations in Kir2.1 cause the developmental and episodic electrical phenotypes of Andersen’s syndrome. Cell 2001;105:511–9. - PubMed
-
- Splawski I, Timothy KW, Sharpe LM, et al. Ca(V)1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism. Cell 2004;119:19–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical