

The impact of anatomic manipulations on pharyngeal collapse: results from a computational model of the normal human upper airway
- PMID: 16162725
- PMCID: PMC3500380
- DOI: 10.1378/chest.128.3.1324
The impact of anatomic manipulations on pharyngeal collapse: results from a computational model of the normal human upper airway
Abstract
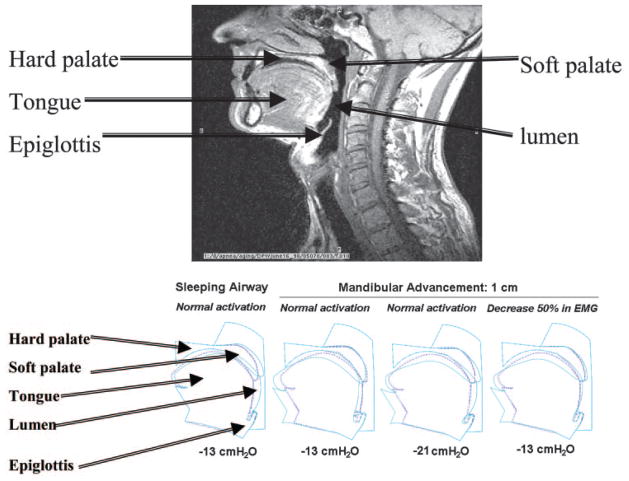
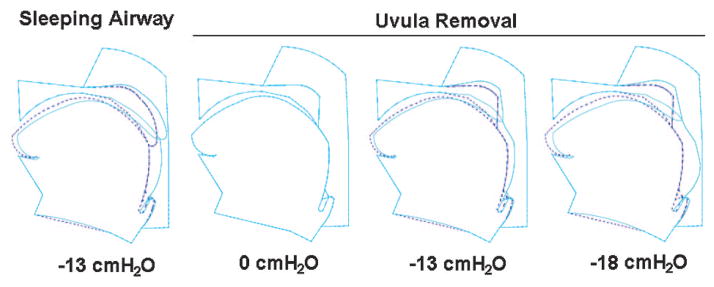
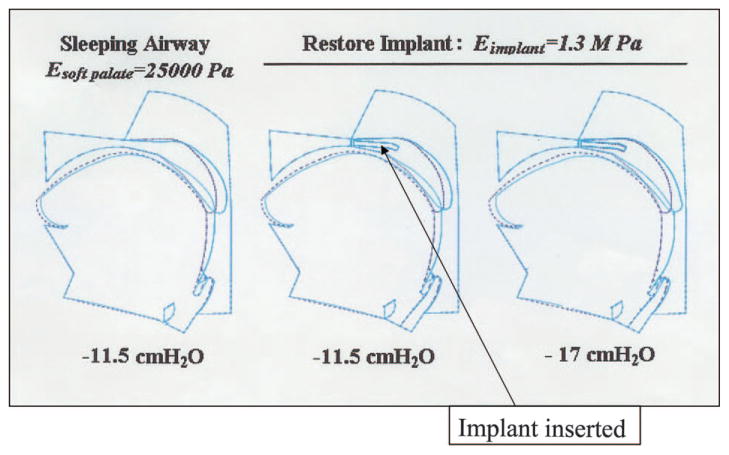
Obstructive sleep apnea (OSA) is a common disease with important neurocognitive and cardiovascular sequelae. Existing therapies are unsatisfactory, leading investigators to seek alternative forms of anatomic manipulation to influence pharyngeal mechanics. We have developed a two-dimensional computational model of the normal human upper airway based on signal averaging of MRI. Using the finite element method, we can perform various anatomic perturbations on the structure in order to assess the impact of these manipulations on pharyngeal mechanics and collapse. By design, the normal sleeping upper airway model collapses at -13 cm H2O. This closing pressure becomes more negative (ie, less collapsible) when we perform mandibular advancement (-21 cm H2O), palatal resection (-18 cm H2O), or palatal stiffening (-17 cm H2O). Where clinical data are available in the literature, the results of our model correspond reasonably well. Furthermore, our model provides information regarding the site of obstruction and provides hypotheses for clinical studies that can be undertaken in the future (eg, combination therapies). We believe that, in the future, finite element modeling will provide a useful tool to help advance our understanding of OSA and its response to various therapies.
Figures
References
-
- Malhotra A, White D. Seminar: obstructive sleep apnoea. Lancet. 2002;360:237–245. - PubMed
-
- Peppard P, Young T, Palta M, et al. Prospective study of the association between sleep disordered breathing and hypertension. N Engl J Med. 2000;342:1378–1384. - PubMed
-
- Jenkinson C, Davies RJ, Mullins R, et al. Comparison of therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised prospective parallel trial. Lancet. 1999;353:2100–2105. - PubMed
-
- Faccenda JF, Mackay TW, Boon NA, et al. Randomized placebo-controlled trial of continuous positive airway pressure on blood pressure in the sleep apnea-hypopnea syndrome. Am J Respir Crit Care Med. 2001;163:344–348. - PubMed
-
- Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, et al. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet. 2002;359:204–210. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
