

Mild dilated cardiomyopathy and increased left ventricular mass predict mortality: the prospective P2C2 HIV Multicenter Study
- PMID: 16169321
- PMCID: PMC4414122
- DOI: 10.1016/j.ahj.2005.06.012
Mild dilated cardiomyopathy and increased left ventricular mass predict mortality: the prospective P2C2 HIV Multicenter Study
Abstract
Background: Many HIV-infected children die with cardiac abnormalities. We sought to understand the course of these HIV-associated abnormalities and their impact on all-cause mortality.
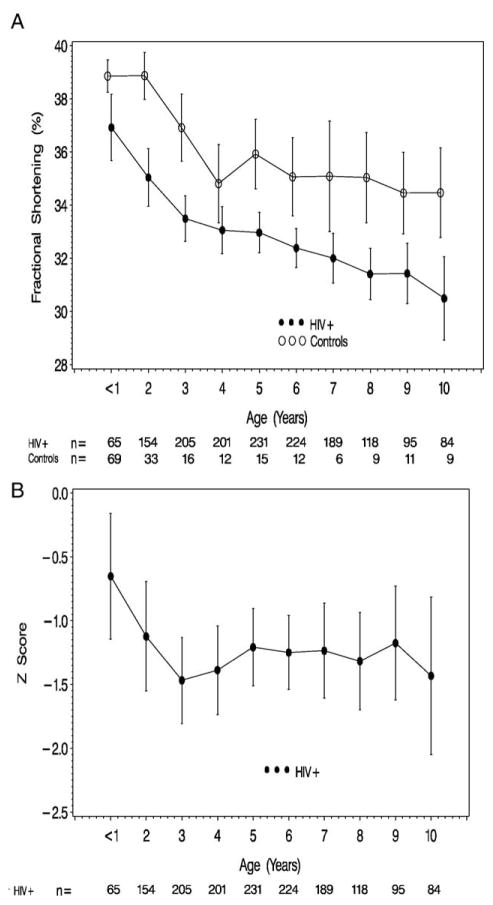
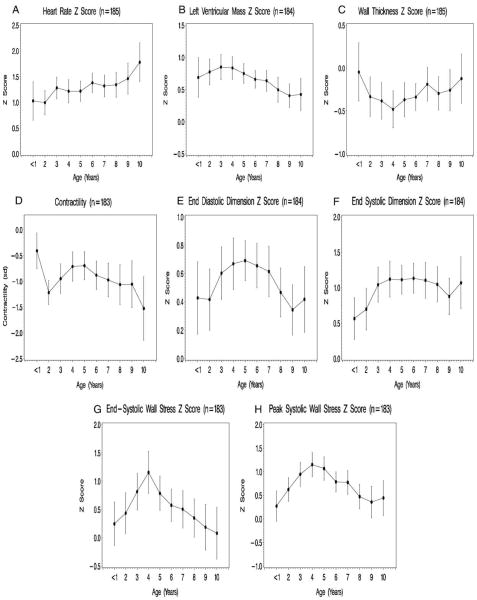
Methods: We describe longitudinal changes in left ventricular (LV) structure and function and mortality in 185 children vertically infected with HIV. Serial cardiac data were obtained from 0.1 to 10 years of age. Age- or body surface area-adjusted z scores were calculated for 10 echocardiographic outcomes.
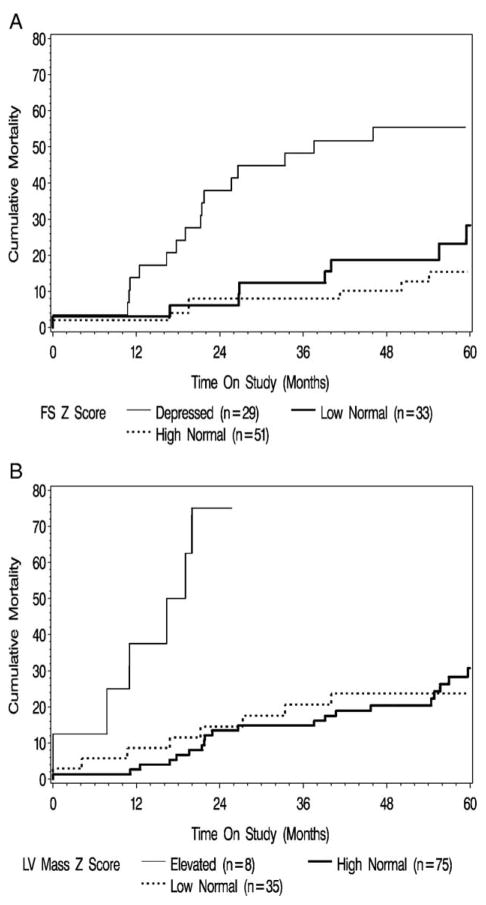
Results: Median age at first echocardiogram was 2 years (range 0.2-9.4 years); median follow-up was 3.6 years (range 0-6.3 years). The 5-year cumulative incidence of congestive heart failure was 12.3%. Mean fractional shortening z scores declined from -0.65 at 1 year of age to -1.47 at 3 years of age without further decline between 3 and 10 years of age. Among children with 2 echocardiograms performed in the first year of follow-up, mild LV dysfunction (fractional shortening of < -2 SD on both echocardiograms) was present in 29 (18%) of 158 children. For these 29 children, the 5-year mortality was 55.4%. Left ventricular mass z scores were elevated at 1 year (mean z score 0.68, P < .001) and remained elevated throughout follow-up. In the 8 children with LV mass z score of > 2 SD on both initial and follow-up echocardiograms, the 5-year mortality was 75%.
Conclusion: In HIV-infected children, LV structure and function progressively deteriorated in the first 3 years of life, resulting in subsequent persistent mild LV dysfunction and increased LV mass. Chronic mild depression of LV function and elevated LV mass were associated with higher all-cause mortality.
Figures
References
-
- Al-Attar I, Orav EJ, Exil V, et al. Predictors of cardiac morbidity and related mortality in children with the acquired immunodeficiency syndrome. J Am Coll Cardiol. 2003;41:1598– 605. - PubMed
Publication types
MeSH terms
Grants and funding
- K01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000645/RR/NCRR NIH HHS/United States
- RR-00043/RR/NCRR NIH HHS/United States
- N01-HR-96039/HR/NHLBI NIH HHS/United States
- N01-HR-96040/HR/NHLBI NIH HHS/United States
- RR-00071/RR/NCRR NIH HHS/United States
- M01 RR000865/RR/NCRR NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- N01 HR096037/HR/NHLBI NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- RR-00188/RR/NCRR NIH HHS/United States
- RR-00533/RR/NCRR NIH HHS/United States
- RR-00645/RR/NCRR NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- RR-00865/RR/NCRR NIH HHS/United States
- N01-HR-96042/HR/NHLBI NIH HHS/United States
- N01-HR-96038/HR/NHLBI NIH HHS/United States
- N01-HR-96041/HR/NHLBI NIH HHS/United States
- N01 HR096043/HR/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
