

Familial hypercholesterolaemia commonly presents with Achilles tenosynovitis
- PMID: 16176995
- PMCID: PMC1798051
- DOI: 10.1136/ard.2005.040766
Familial hypercholesterolaemia commonly presents with Achilles tenosynovitis
Abstract
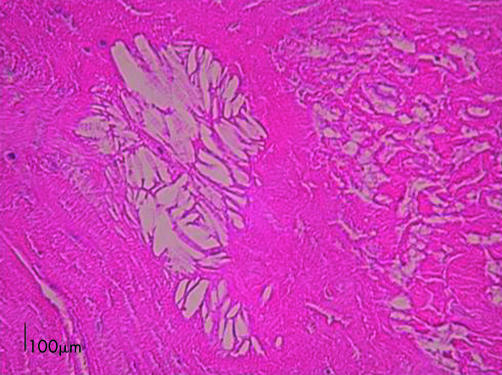
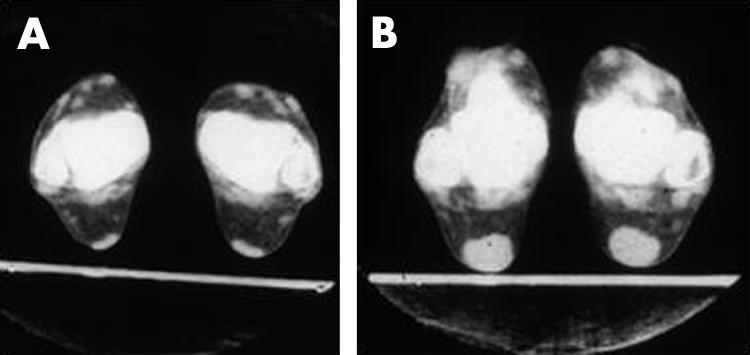
Background: Patients with heterozygous familial hypercholesterolaemia (HeFH) develop tendon xanthomata (TX), most commonly in their Achilles tendons. Even before tendons are chronically enlarged, tenosynovitis may occur and medical advice be sought. Untreated HeFH carries a high risk of premature coronary heart disease, which can be ameliorated by early diagnosis.
Objective: To determine the prevalence of episodes of Achilles tendon pain in HeFH before its diagnosis.
Methods: Patients with definite HeFH (Simon Broome criteria) attending a lipid clinic were identified. They completed a questionnaire asking about symptoms relating to their Achilles tendons. Unaffected spouses or cohabiting partners served as controls.
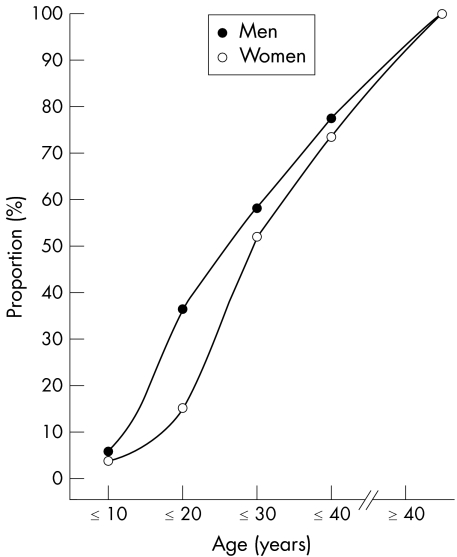
Results: 133 patients (47% men) and 87 controls (51% men) participated. TX had been recognised by the referring physicians in <5% of cases. However, 62 (46.6% (95% confidence interval (CI) 38.1 to 55.1)) patients had experienced one or more episodes of pain in one or both Achilles tendons lasting >3 days, whereas only 6 (6.9% (1.6 to 12.2)) controls had done so (difference p<0.001; likelihood ratio 6.75). Typically, in the patients with HeFH the pain lasted 4 days (median). It was described as severe or very severe in 24/62 (38.7% (30.4 to 47.0)) patients with HeFH, but never more than moderate in controls. 35 (26.3% (18.8 to 33.8)) patients with HeFH had consulted a doctor about Achilles tendon pain, but in no case had this led to a diagnosis of HeFH. None of the controls had consulted a doctor.
Conclusions: Measurement of serum cholesterol in patients presenting with painful Achilles tendon could lead to early diagnosis of HeFH.
Conflict of interest statement

References
-
- Goldstein J L, Brown M D. Familial hypercholesterolaemia, In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of inherited disease. 8th ed. New York: McGraw‐Hill, 20012863–2913.
-
- Marks D, Thorogood M, Neil H A W, Humphries S E. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis 20031681–14. - PubMed
-
- Neil H A W, Hawkins M M, Durrington P N, Betteridge D J, Capps N, Humphries S E. Non‐coronary heart disease mortality and risk of fatal cancer in patients with treated heterozygous familial hypercholesterolaemia: a prospective study. Atherosclerosis 2005179293–297. - PubMed
-
- Talmud P, Tybjaerg‐Hansen A, Bhatnagar D, MBewu A D, Durrington P N, Miller J P.et al Screening for specific mutations in patients with a clinical diagnosis of familial hypercholesterolaemia. Atherosclerosis 199189137–142. - PubMed
-
- Myant N B, Slack J. Type II hyperlipoproteinaemia. Clin Endocrinol Metab 1973281–109. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
