

Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis
- PMID: 16179995
- PMCID: PMC3489325
- DOI: 10.1007/s00586-005-0984-5
Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis
Abstract
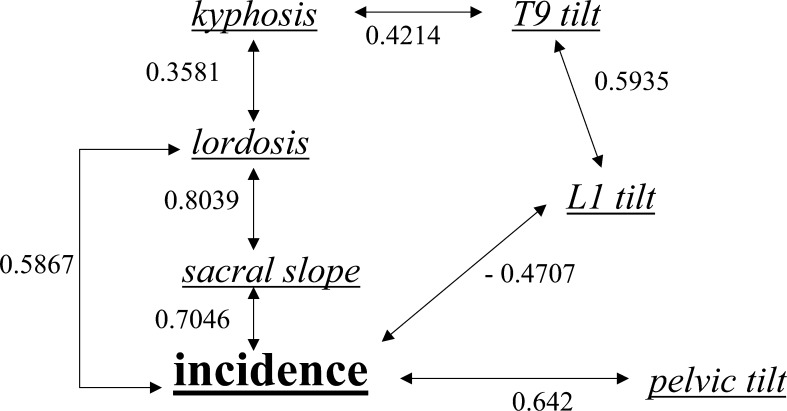
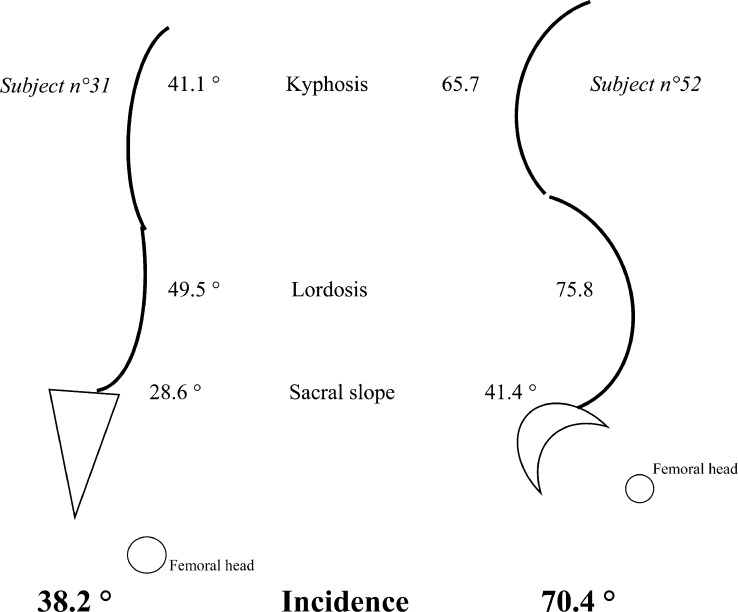
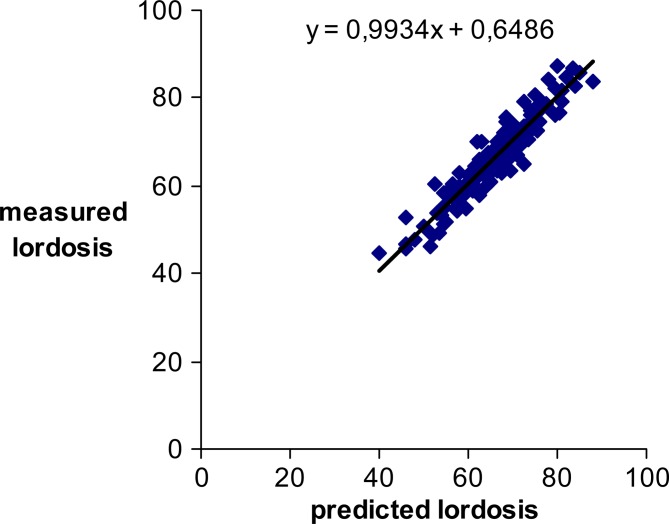
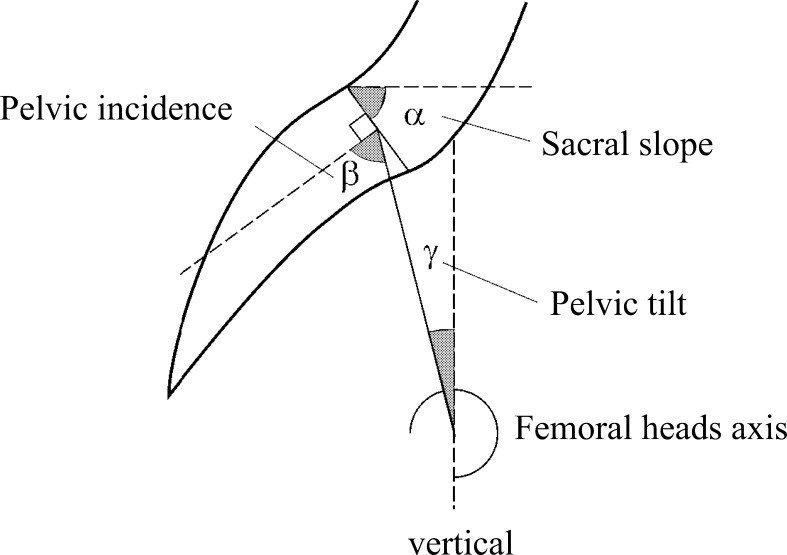
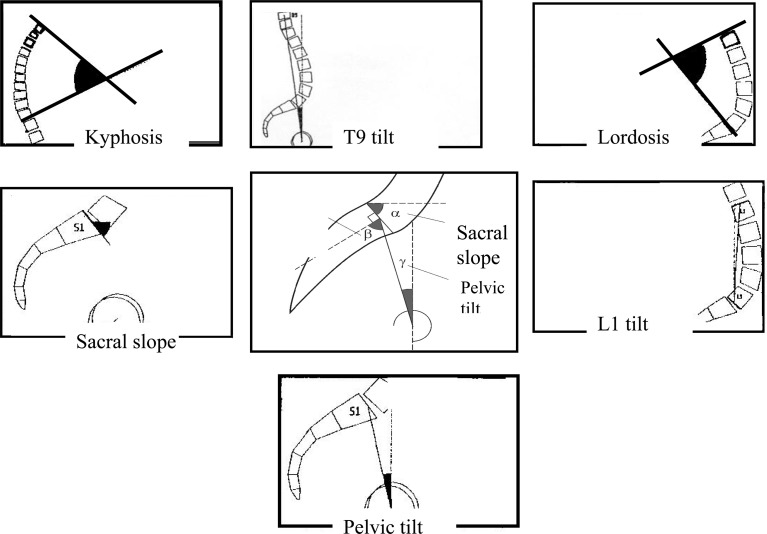
Pelvis and spinal curves were studied with an angular parameter typical of pelvis morphology: pelvic incidence. A significant chain of correlations between positional pelvic and spinal parameters and incidence is known. This study investigated standards of incidence and a predictive equation of lordosis from selective pelvic and spinal individual parameters. One hundred and forty nine (78 men and 71 women) healthy adults, aged 19-50 years, with no spinal disorders, were included and had a full-spine lateral X-ray in a standardised upright position. Computerised technology was used for the measurement of angular parameters. Mean-deviation section of each parameter and Pearson correlation test were calculated. A multivariate selection algorithm was running with the lordosis (predicted variable) and the other spinal and pelvic parameters (predictor variables), to determine the best sets of predictors to include in the model. A low incidence (<44 degrees ) decreased sacral-slope and the lordosis is flattened. A high incidence (>62 degrees ) increased sacral-slope and the lordosis is more pronounced. Lordosis predictive equation is based on incidence, kyphosis, sacral-slope and +/-T9 tilt. The confidence limits and the residuals (the difference between measured and predicted lordosis) assessed the predicted lordosis accuracy of the model: respectively, +/-1.65 and 2.41 degrees with the 4-item model; +/-1.73 and 3.62 degrees with the 3-item model. The ability of the functional spine-pelvis unit to search for a sagittal balance depended both on the incidence and on the variation section of the other positional parameters. Incidence gave an adaptation potential at two levels of positional compensation: overlying state (kyphosis, T9 tilt), underlying state (sacral slope, pelvic tilt). The biomechanical and clinical conditions of the standing posture (as in scoliosis, low back pain, spondylisthesis, spine surgery, obesity and postural impairments) can be studied by comparing the measured lordosis with the predicted lordosis.
Figures
References
-
- Boisaubert B, Montigny JP, Duval-Beaupere G, Hecquet J, Marty C. Incidence pelvienne, sacrum et spondylolisthésis. Rachis. 1997;9:187–192.
-
- Boulay Anatomical reliability of two fundamental radiological and clinical pelvic. 2005;parameters:incidence.
-
- Descamps H, Commare MC, Marty C, Duval-Beaupere G. Le paramètre Incidence chez le petit enfant. Rachis. 1996;8:177–180.
-
- Descamps H, Commare MC, Marty C, Hecquet J, Duval-Beaupere G. Modifications des angles pelviens, dont l’Incidence pelvienne, au cours de la croissance humaine. Biom Hum et Anthropol. 1999;17:59–63.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
