

Fat distribution in men with HIV infection
- PMID: 16186728
- PMCID: PMC3166344
- DOI: 10.1097/01.qai.0000182230.47819.aa
Fat distribution in men with HIV infection
Abstract
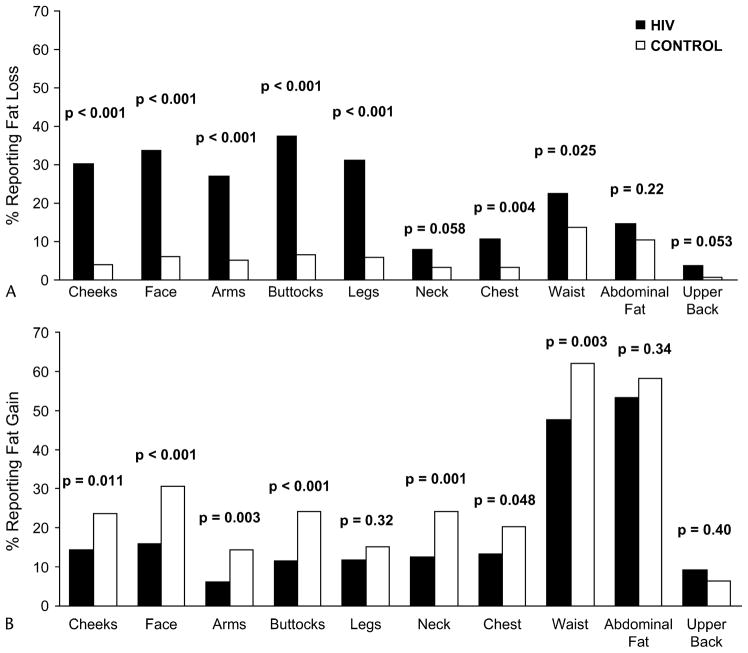
Objective: Both peripheral fat loss and central fat gain have been reported in HIV infection. Which changes are specific to HIV were determined by comparison with control subjects and the associations among different adipose tissue depots were determined.
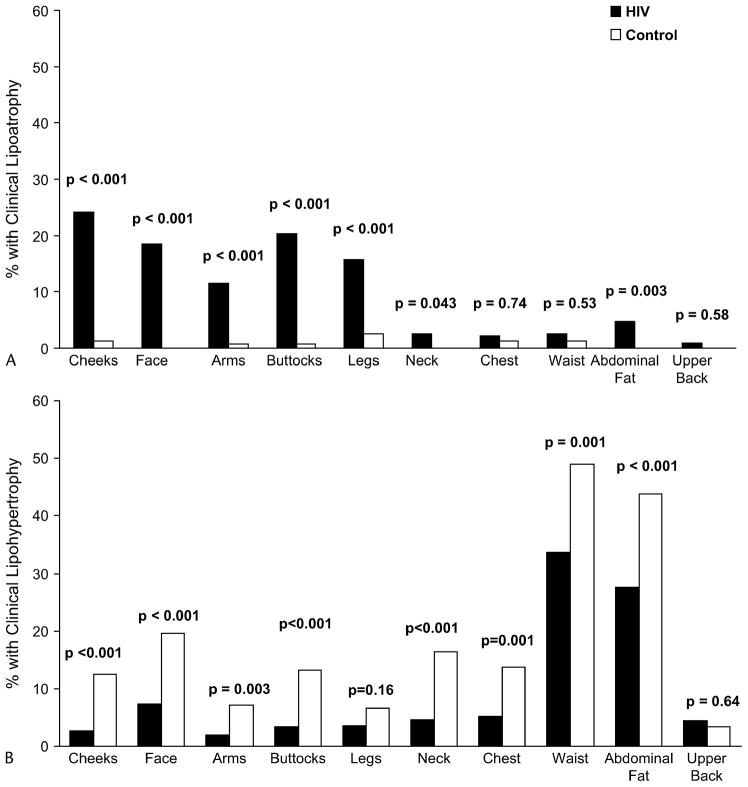
Methods: Cross-sectional analysis of HIV-positive and control men from the study of Fat Redistribution and Metabolic Change in HIV Infection. Lipoatrophy or lipohypertrophy was defined as concordance between participant report of change and examination. Regional adipose tissue volume was measured by magnetic resonance imaging (MRI).
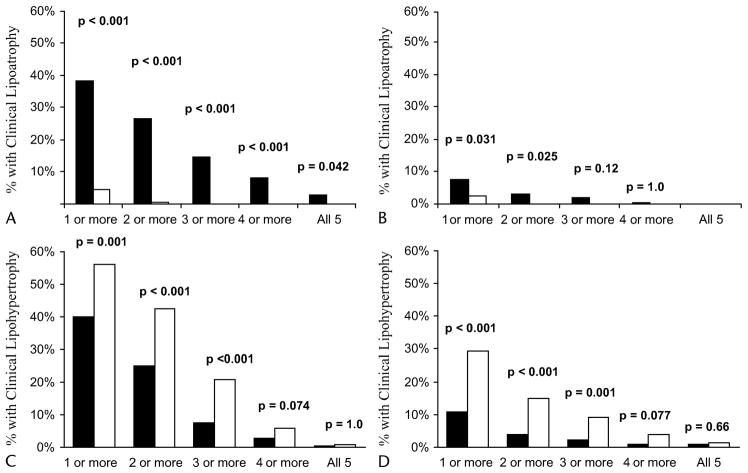
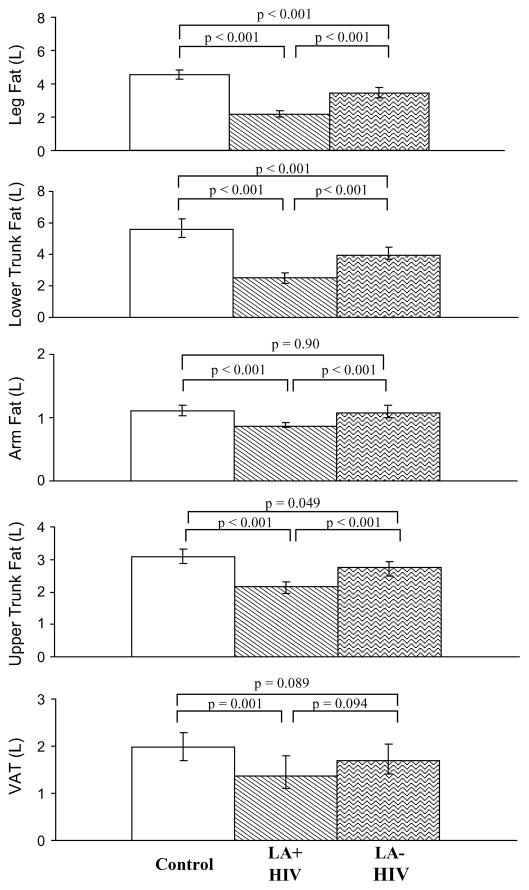
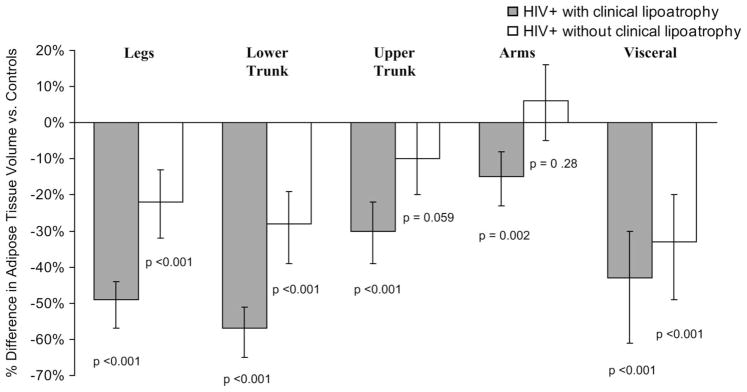
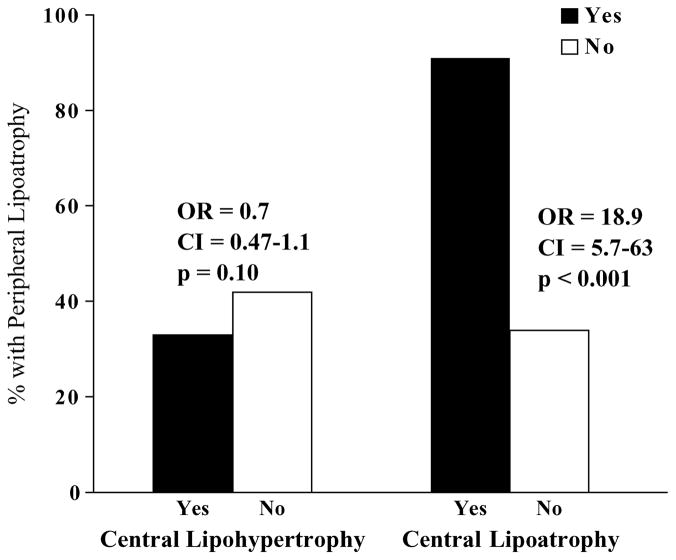
Results: HIV-positive men reported more fat loss than controls in all peripheral and most central depots. Peripheral lipoatrophy was more frequent in HIV-positive men than in controls (38.3% vs. 4.6%, P < 0.001), whereas central lipohypertrophy was less frequent (40.2% vs. 55.9%, P = 0.001). Among HIV-positive men, the presence of central lipohypertrophy was not positively associated with peripheral lipoatrophy (odds ratio = 0.71, CI: 0.47 to 1.06, P = 0.10). On MRI, HIV-positive men with clinical peripheral lipoatrophy had less subcutaneous adipose tissue (SAT) in peripheral and central sites and less visceral adipose tissue (VAT) than HIV-positive men without peripheral lipoatrophy. HIV-positive men both with and without lipoatrophy had less SAT than controls, with legs and lower trunk more affected than upper trunk. Use of the antiretroviral drugs stavudine or indinavir was associated with less leg SAT but did not appear to be associated with more VAT; nevirapine use was associated with less VAT.
Conclusion: Both peripheral and central subcutaneous lipoatrophy was found in HIV infection. Lipoatrophy in HIV-positive men is not associated with reciprocally increased VAT.
Figures
Comment in
-
Morphologic changes in HIV-infected men: sorting fact from fiction.J Acquir Immune Defic Syndr. 2005 Oct 1;40(2):119-20. doi: 10.1097/01.qai.0000187137.34789.dd. J Acquir Immune Defic Syndr. 2005. PMID: 16186727 No abstract available.
References
-
- Safrin S, Grunfeld C. Fat distribution and metabolic changes in patients with HIV infection. AIDS. 1999;13:2493–2505. - PubMed
-
- Lo JC, Mulligan K, Tai VW, et al. “Buffalo hump” in men with HIV-1 infection. Lancet. 1998;351:867–870. - PubMed
-
- Miller KD, Jones E, Yanovski JA, et al. Visceral abdominal-fat accumulation associated with use of indinavir. Lancet. 1998;351:871–875. - PubMed
-
- Miller KK, Daly PA, Sentochnik D, et al. Pseudo-Cushing’s syndrome in human immunodeficiency virus-infected patients. Clin Infect Dis. 1998;27:68–72. - PubMed
-
- Viraben R, Aquilina C. Indinavir-associated lipodystrophy. AIDS. 1998;12:F37–F39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- RR00865/RR/NCRR NIH HHS/United States
- HL74814/HL/NHLBI NIH HHS/United States
- M01 RR000865/RR/NCRR NIH HHS/United States
- RR00051/RR/NCRR NIH HHS/United States
- M01 RR000054/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- RR00052/RR/NCRR NIH HHS/United States
- R01 HL074814/HL/NHLBI NIH HHS/United States
- RR0636/RR/NCRR NIH HHS/United States
- RR00054/RR/NCRR NIH HHS/United States
- AI 027767/AI/NIAID NIH HHS/United States
- R01-DK57508/DK/NIDDK NIH HHS/United States
- R01 DK057508/DK/NIDDK NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- HL 53359/HL/NHLBI NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- M01-RR00036/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
