

Effect of artemether-lumefantrine policy and improved vector control on malaria burden in KwaZulu-Natal, South Africa
- PMID: 16187798
- PMCID: PMC1240068
- DOI: 10.1371/journal.pmed.0020330
Effect of artemether-lumefantrine policy and improved vector control on malaria burden in KwaZulu-Natal, South Africa
Abstract
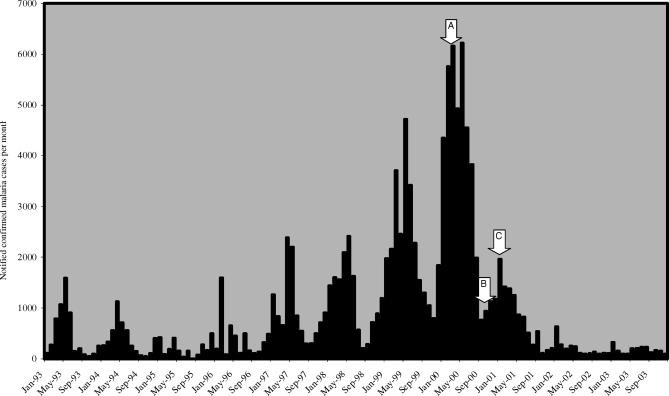
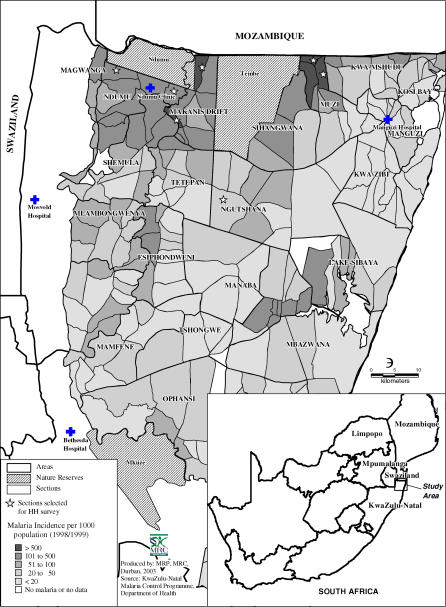
Background: Between 1995 and 2000, KwaZulu-Natal province, South Africa, experienced a marked increase in Plasmodium falciparum malaria, fuelled by pyrethroid and sulfadoxine-pyrimethamine resistance. In response, vector control was strengthened and artemether-lumefantrine (AL) was deployed in the first Ministry of Health artemisinin-based combination treatment policy in Africa. In South Africa, effective vector and parasite control had historically ensured low-intensity malaria transmission. Malaria is diagnosed definitively and treatment is provided free of charge in reasonably accessible public-sector health-care facilities.
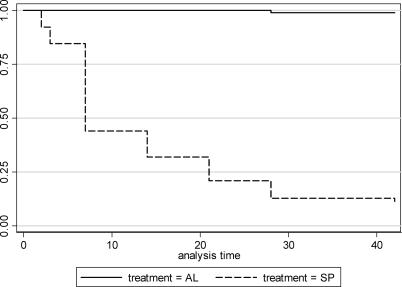
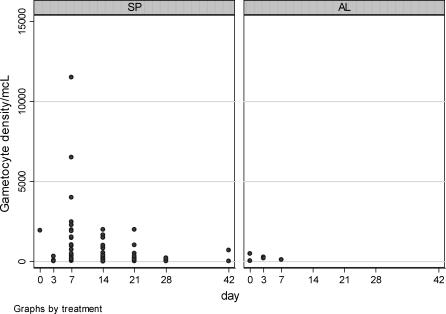
Methods and findings: We reviewed four years of malaria morbidity and mortality data at four sentinel health-care facilities within KwaZulu-Natal's malaria-endemic area. In the year following improved vector control and implementation of AL treatment, malaria-related admissions and deaths both declined by 89%, and outpatient visits decreased by 85% at the sentinel facilities. By 2003, malaria-related outpatient cases and admissions had fallen by 99%, and malaria-related deaths had decreased by 97%. There was a concomitant marked and sustained decline in notified malaria throughout the province. No serious adverse events were associated causally with AL treatment in an active sentinel pharmacovigilance survey. In a prospective study with 42 d follow up, AL cured 97/98 (99%) and prevented gametocyte developing in all patients. Consistent with the findings of focus group discussions, a household survey found self-reported adherence to the six-dose AL regimen was 96%.
Conclusion: Together with concurrent strengthening of vector control measures, the antimalarial treatment policy change to AL in KwaZulu-Natal contributed to a marked and sustained decrease in malaria cases, admissions, and deaths, by greatly improving clinical and parasitological cure rates and reducing gametocyte carriage.
Conflict of interest statement
Figures
Comment in
-
Rolling back a malaria epidemic in South Africa.PLoS Med. 2005 Nov;2(11):e368. doi: 10.1371/journal.pmed.0020368. Epub 2005 Oct 4. PLoS Med. 2005. PMID: 16187736 Free PMC article.
References
-
- Trape JF, Pison G, Preziosi MP, Desgrees du Lou A, Delaunay V, et al. Impact of chloroquine resistance on malaria mortality. C R Acad Sci III. 1998;321:689–697. - PubMed
-
- Snow W, Trape J, Marsh K. The past, present and future of childhood malaria mortality in Africa. Trends in Parasitol. 2001;17:593–597. - PubMed
-
- Hargreaves K, Koekemoer LL, Brooke BD, Runt RH, Mthembu J, et al. Anopholes funestus resistant to pyrethroid insecticides in South Africa. Med Vet Entomol. 2000;14:181–189. - PubMed
-
- Vaughan-Williams CH. Success of insecticide spraying in controlling malaria [letter] S Afr Med J. 2003;93:160. - PubMed
-
- Bredenkamp BLF, Sharp BL, Mthembu SD, Durrheim DN, Barnes KI. Failure of sulfadoxine-pyrimethamine in treating Plasmodium falciparum malaria in KwaZulu–Natal. S Afr Med J. 2001;91:970–972. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
