

Improved survival of ischemic cutaneous and musculocutaneous flaps after vascular endothelial growth factor gene transfer using adeno-associated virus vectors
- PMID: 16192634
- PMCID: PMC1603677
- DOI: 10.1016/S0002-9440(10)61188-1
Improved survival of ischemic cutaneous and musculocutaneous flaps after vascular endothelial growth factor gene transfer using adeno-associated virus vectors
Abstract
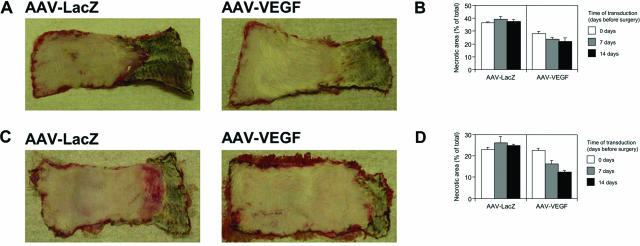
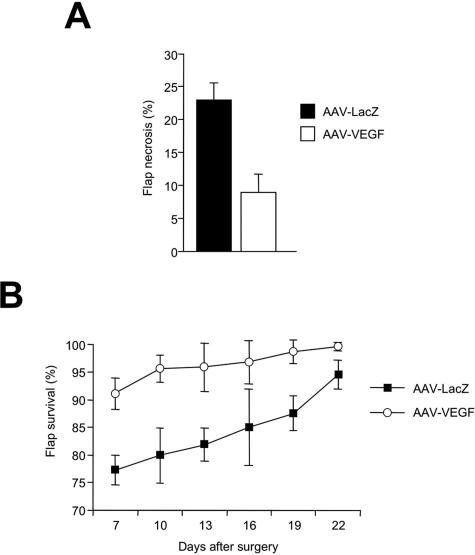
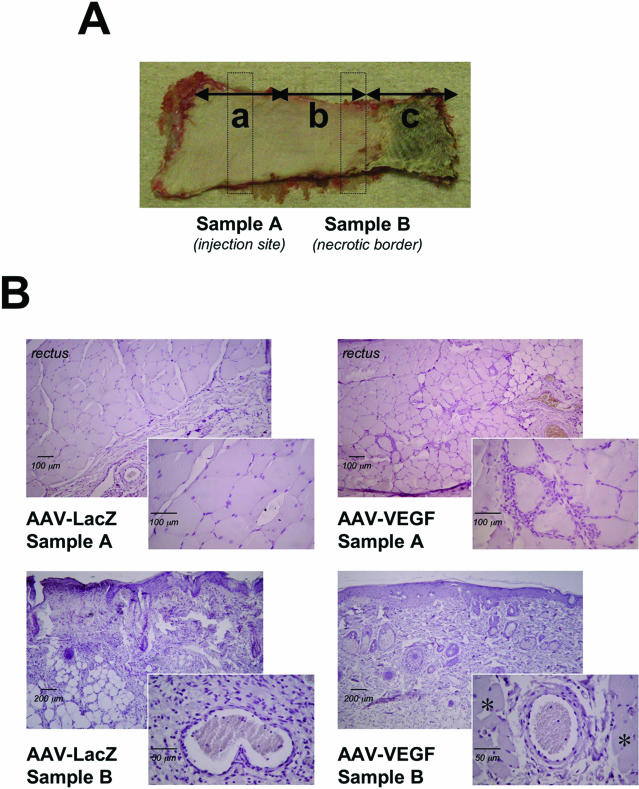
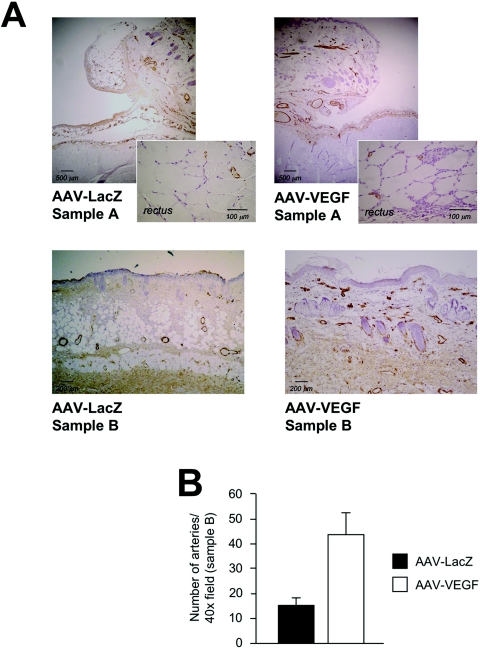
A major challenge in reconstructive surgery is flap ischemia, which might benefit from induction of therapeutic angiogenesis. Here we demonstrate the effect of an adeno-associated virus (AAV) vector delivering vascular endothelial growth factor (VEGF)165 in two widely recognized in vivo flap models. For the epigastric flap model, animals were injected subcutaneously with 1.5 x 10(11) particles of AAV-VEGF at day 0, 7, or 14 before flap dissection. In the transverse rectus abdominis musculocutaneous flap model, AAV-VEGF was injected intramuscularly. The delivery of AAV-VEGF significantly improved flap survival in both models, reducing necrosis in all treatment groups compared to controls. The most notable results were obtained by administering the vector 14 days before flap dissection. In the transverse rectus abdominis musculocutaneous flap model, AAV-VEGF reduced the necrotic area by >50% at 1 week after surgery, with a highly significant improvement in the healing process throughout the following 2 weeks. The therapeutic effect of AAV-VEGF on flap survival was confirmed by histological evidence of neoangiogenesis in the formation of large numbers of CD31-positive capillaries and alpha-smooth muscle actin-positive arteriolae, particularly evident at the border between viable and necrotic tissue. These results underscore the efficacy of VEGF-induced neovascularization for the prevention of tissue ischemia and the improvement of flap survival in reconstructive surgery.
Figures


Similar articles
-
Improved survival of rat ischemic cutaneous and musculocutaneous flaps after VEGF gene transfer.Microsurgery. 2007;27(5):439-45. doi: 10.1002/micr.20378. Microsurgery. 2007. PMID: 17596844
-
Enhancement of flap survival and changes in angiogenic gene expression after AAV2-mediated VEGF gene transfer to rat ischemic flaps.Wound Repair Regen. 2011 Jul-Aug;19(4):498-504. doi: 10.1111/j.1524-475X.2011.00705.x. Epub 2011 Jun 7. Wound Repair Regen. 2011. PMID: 21649787
-
Delivery of FGF-2 but not VEGF by encapsulated genetically engineered myoblasts improves survival and vascularization in a model of acute skin flap ischemia.Gene Ther. 2001 Apr;8(7):523-33. doi: 10.1038/sj.gt.3301436. Gene Ther. 2001. PMID: 11319619
-
Acute and sustained effects of vascular endothelial growth factor on survival of flaps and skin grafts.Ann Plast Surg. 2011 May;66(5):581-2. doi: 10.1097/SAP.0b013e3182057376. Ann Plast Surg. 2011. PMID: 21451385 Review.
-
[Therapeutic angiogenesis for ischemic heart disease induced by gene transfer].Nihon Rinsho. 2005 Dec;63 Suppl 12:588-93. Nihon Rinsho. 2005. PMID: 16416858 Review. Japanese. No abstract available.
Cited by
-
Bone marrow cells recruited through the neuropilin-1 receptor promote arterial formation at the sites of adult neoangiogenesis in mice.J Clin Invest. 2008 Jun;118(6):2062-75. doi: 10.1172/JCI32832. J Clin Invest. 2008. PMID: 18483621 Free PMC article.
-
Fibroblast Growth Factor-1 vs. Fibroblast Growth Factor-2 in Ischemic Skin Flap Survival in a Rat Animal Model.World J Plast Surg. 2016 Sep;5(3):274-279. World J Plast Surg. 2016. PMID: 27853691 Free PMC article.
-
Biologic Brachytherapy: Genetically Modified Surgical Flap as a Therapeutic Tool-A Systematic Review of Animal Studies.Int J Mol Sci. 2024 Sep 25;25(19):10330. doi: 10.3390/ijms251910330. Int J Mol Sci. 2024. PMID: 39408659 Free PMC article.
-
VEGF and Other Gene Therapies Improve Flap Survival-A Systematic Review and Meta-Analysis of Preclinical Studies.Int J Mol Sci. 2024 Feb 23;25(5):2622. doi: 10.3390/ijms25052622. Int J Mol Sci. 2024. PMID: 38473869 Free PMC article.
-
Overexpressed HIF-2α in Endothelial Cells Promotes Vascularization and Improves Random Pattern Skin Flap Survival.Plast Reconstr Surg Glob Open. 2014 May 7;2(4):e132. doi: 10.1097/GOX.0000000000000083. eCollection 2014 Apr. Plast Reconstr Surg Glob Open. 2014. PMID: 25289325 Free PMC article.
References
-
- Hallock GG. Physiological studies using laser Doppler flowmetry to compare blood flow to the zones of the free TRAM flap. Ann Plast Surg. 2001;47:229–233. - PubMed
-
- Machens HG, Salehi J, Weich H, Munch S, Siemers F, Krapohl BD, Herter KH, Kruger S, Reichert B, Berger A, Vogt P, Mailander P. Angiogenic effects of injected VEGF165 and sVEGFR-1 (sFLT-1) in a rat flap model. J Surg Res. 2003;111:136–142. - PubMed
-
- Padubidri A, Browne E., Jr Effect of vascular endothelial growth factor (VEGF) on survival of random extension of axial pattern skin flaps in the rat. Ann Plast Surg. 1996;37:604–611. - PubMed
-
- Li QF, Reis ED, Zhang WX, Silver L, Fallon JT, Weinberg H. Accelerated flap prefabrication with vascular endothelial growth factor. J Reconstr Microsurg. 2000;16:45–49. - PubMed
-
- Kryger Z, Dogan T, Zhang F, Komorowska-Timek E, Shi DY, Cheng C, Lineaweaver WC, Buncke HJ. Effects of VEGF administration following ischemia on survival of the gracilis muscle flap in the rat. Ann Plast Surg. 1999;43:172–178. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
