

T1 adenocarcinoma of the rectum: transanal excision or radical surgery?
- PMID: 16192807
- PMCID: PMC1402341
- DOI: 10.1097/01.sla.0000183355.94322.db
T1 adenocarcinoma of the rectum: transanal excision or radical surgery?
Abstract
Background: Recent studies suggest local excision may be acceptable treatment of T1 adenocarcinoma of the rectum, but there is little comparative data with radical surgery to assess outcomes and quantify risk. We performed a retrospective evaluation of patients with T1 rectal cancers treated by either transanal excision or radical resection at our institution to assess patient selection, cancer recurrence, and survival.
Methods: All patients who underwent surgery for T1 adenocarcinomas of the rectum (0-15 cm from anal verge) by either transanal excision (TAE) or radical resection (RAD) between January 1987 and January 2004 were identified from a prospective database. Data were analyzed using Fisher exact test, Kaplan-Meier method, and log-rank test.
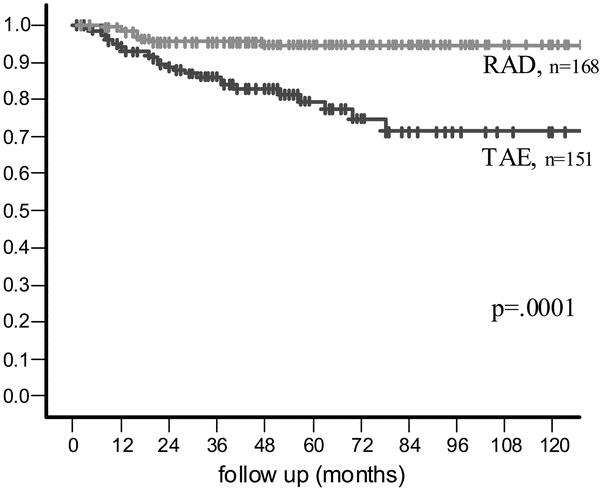
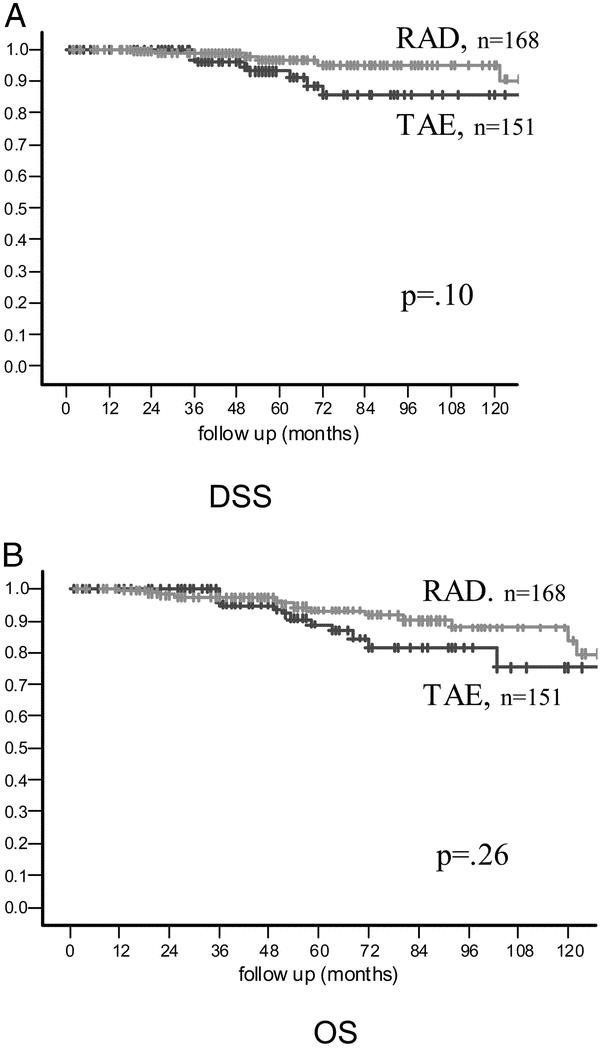
Results: Three hundred nineteen consecutive patients with T1 lesions were treated by transanal excision (n = 151) or radical surgery (n = 168) over the 17-year period. RAD surgery was associated with higher tumor location in the rectum, slightly larger tumor size, a similar rate of adverse histology, and a lymph node metastasis rate of 18%. Despite these features, patients who underwent RAD surgery had fewer local recurrences, fewer distant recurrences, and significantly better recurrence-free survival (P = 0.0001). Overall and disease-specific survival was similar for RAD and TAE groups.
Conclusion: Despite a similar risk profile in the 2 surgical groups, patients with T1 rectal cancer treated by local excision were observed to have a 3- to 5-fold higher risk of tumor recurrence compared with patients treated by radical surgery. Local excision should be reserved for low-risk cancers in patients who will accept an increased risk of tumor recurrence, prolonged surveillance, and possible need for aggressive salvage surgery. Radical resection is the more definitive surgical treatment of T1 rectal cancers.
Figures
Comment in
-
T1 adenocarcinoma of the rectum: transanal excision or radical surgery?Ann Surg. 2007 Feb;245(2):338-9. doi: 10.1097/01.sla.0000253076.01085.fd. Ann Surg. 2007. PMID: 17245194 Free PMC article. No abstract available.
References
-
- Steele GD Jr, Herndon JE, Bleday R, et al. Sphincter-sparing treatment for distal rectal adenocarcinoma. Ann Surg Oncol. 1999;6:433–441. - PubMed
-
- Bleday R, Breen E, Jessup JM, et al. Prospective evaluation of local excision for small rectal cancers. Dis Colon Rectum. 1997;40:388–392. - PubMed
-
- Kim HK, Jessup JM, Beard CJ, et al. Locally advanced rectal carcinoma: pelvic control and morbidity following preoperative radiation therapy, resection, and intraoperative radiation therapy. Int J Radiat Oncol Biol Phys. 1997;38:777–783. - PubMed
-
- Rothenberger DA, Garcia-Aguilar J. Role of local excision in the treatment of rectal cancer. Semin Surg Oncol. 2000;19:367–375. - PubMed
-
- Kim DG, Madoff RD. Transanal treatment of rectal cancer: ablative methods and open resection. Semin Surg Oncol. 1998;15:101–113. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
