

100 multivisceral transplants at a single center
- PMID: 16192808
- PMCID: PMC1402343
- DOI: 10.1097/01.sla.0000183347.61361.7a
100 multivisceral transplants at a single center
Abstract
Objective: The objective of this study was to summarize the evolution of multivisceral transplantation over a decade of experience and evaluate its current status.
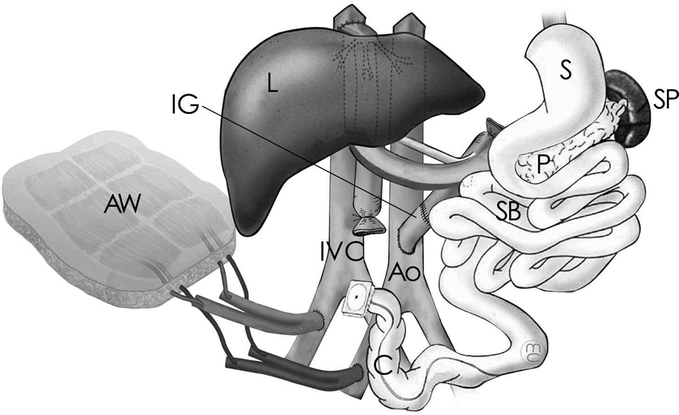
Summary background data: Multivisceral transplantation can be valuable for the treatment of patients with massive abdominal catastrophes. Its major limitations have been technical and rejection of the intestinal graft.
Methods: This study consisted of an outcome analysis of 98 consecutive patients who received multivisceral transplantation at our institution. This represents the largest single center experience to date.
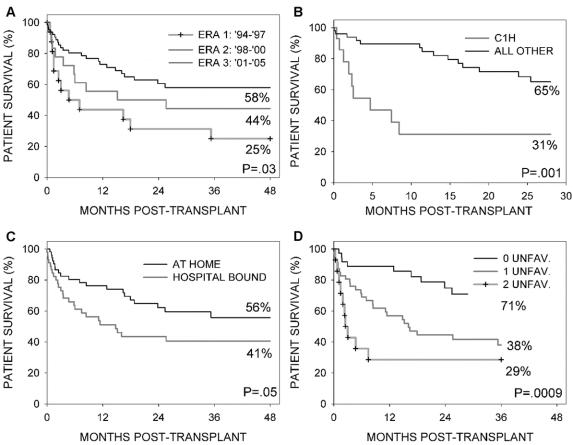
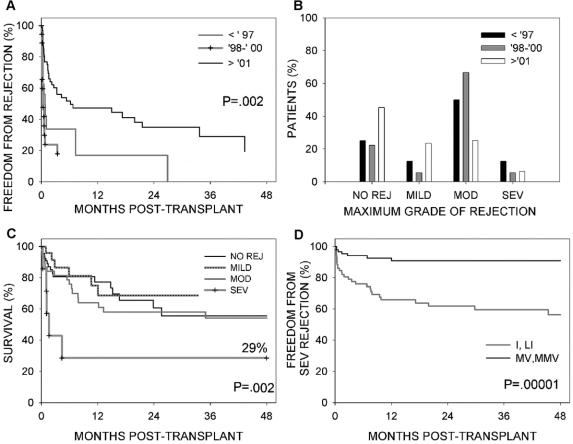
Results: The most common diseases in our population before transplant were intestinal gastroschisis and intestinal dysmotility syndromes in children, and mesenteric thrombosis and trauma in adults. Kaplan Meier estimated patient and graft survivals for all cases were 65% and 63% at 1 year, 49% and 47% at 3 years, and 49% and 47% at 5 years. Factors that adversely influenced patient survival included transplant before 1998 (P = 0.01), being hospitalized at the time of transplant (P = 0.05), and being a child who received Campath-1H induction (P = 0.03). Among 37 patients who had none of these 3 factors (15 adults and 22 children), estimated 1- and 3-year survivals were 89% and 71%, respectively. Patients transplanted since 2001 had significantly less moderate and severe rejections (31.6% vs 67.6%, P = 0.0005) with almost half of these patients never developing rejection.
Conclusions: Multivisceral transplantation is now an effective treatment of patients with complex abdominal pathology. The incidences of serious acute rejection and patient survival have improved in the most recent experience. Our results show that the multivisceral graft seems to facilitate engraftment of transplanted organs and raises the possibility that there is a degree of immunologic protection afforded by this procedure.
Figures
Comment in
-
Immunologic benefits of spleen transplantation in the absence of graft-versus-host disease.Ann Surg. 2006 May;243(5):710-1. doi: 10.1097/01.sla.0000216774.20043.74. Ann Surg. 2006. PMID: 16633012 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
