

Surgeon contribution to hospital bottom line: not all are created equal
- PMID: 16192813
- PMCID: PMC1402352
- DOI: 10.1097/01.sla.0000184693.61680.24
Surgeon contribution to hospital bottom line: not all are created equal
Abstract
Objective: We hypothesized that surgeon productivity is directly related to hospital operating margin, but significant variation in margin contribution exists between specialties.
Summary background data: As the independent practitioner becomes an endangered species, it is critical to better understand the surgeon's importance to a hospital's bottom line. An appreciation of surgeon contribution to hospital profitability may prove useful in negotiations relating to full-time employment or other models.
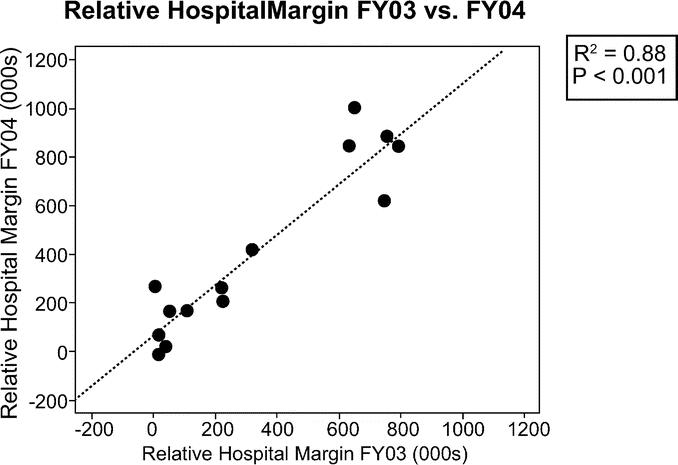
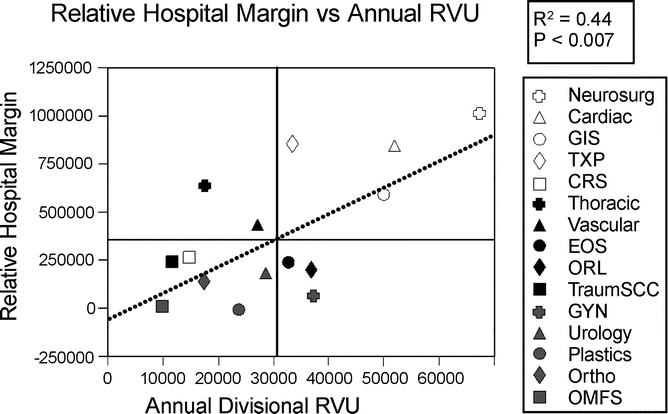
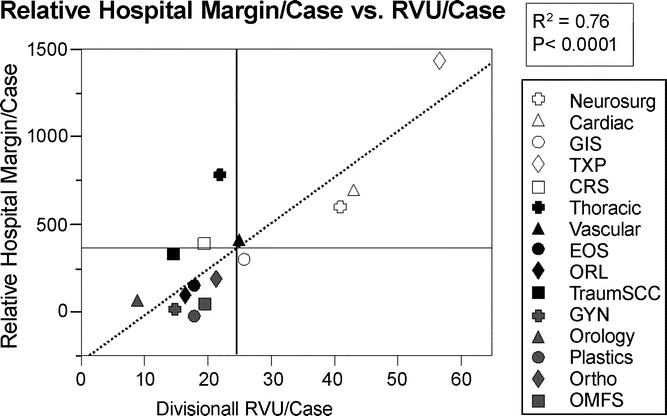
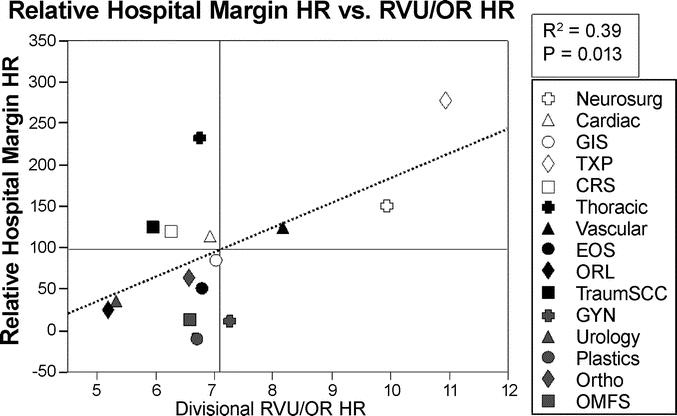
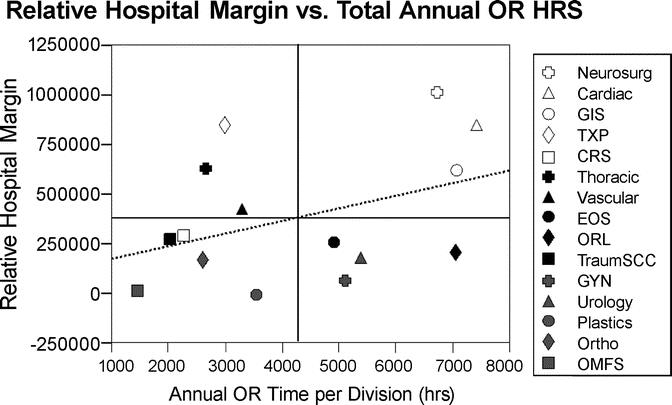
Methods: Surgeon total relative value units (RVUs), a measure of productivity, were collected from operating room (OR) logs. Annual hospital margin per specialty was provided by hospital finance. Hospital margin data were normalized by dividing by a constant such that the highest relative hospital margin (RHM) in fiscal year 2004 expressed as margin units (mu) was 1 million mu. For each specialty, data analyzed included RHM/OR HR, RHM/case, and RHM/RVU.
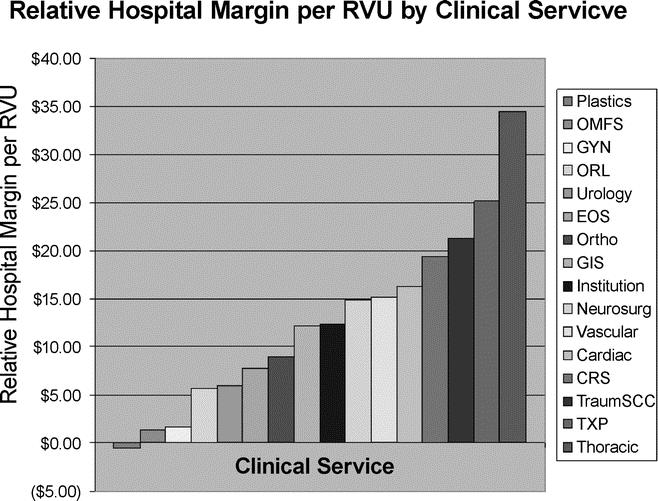
Results: Thoracic (34.55 mu/RVU) and transplant (25.13 mu/RVU) were the biggest contributors to hospital margin. Plastics (-0.57 mu/RVU), maxillofacial (1.41 mu/RVU), and gynecology (1.66 mu/RVU) contributed least to hospital margin. Relative hospital margin per OR HR for transplant slightly exceeded thoracic (275.74 mu vs 233.94 mu) at the top and plastics and maxillofacial contributed the least (-3.83 mu/OR HR vs 9.36 mu/OR HR).
Conclusions: Surgeons contribute significantly to hospital margin with certain specialties being more profitable than others. Payer mix, the penetration of managed care, and negotiated contracts as well as a number of other factors all have an impact on an individual hospital's margin. Surgeons should be fully cognizant of their significant influence in the marketplace.
Figures

Comment in
-
Prior research in measuring financial differences among surgical specialties and using such differences in decision making.Ann Surg. 2006 Nov;244(5):833. doi: 10.1097/01.sla.0000243604.59248.e5. Ann Surg. 2006. PMID: 17060780 Free PMC article. No abstract available.
References
-
- Todd BA, Resnick AS, Stuhlemmer R, et al. Challenges of the 80-hour resident work rules: collaboration between surgeons and nonphysician practitioners. Surg Clin North Am. 2004;84:1573–1586. - PubMed
-
- Taheri PA, Butz DA, Dechert R, et al. How DRGs hurt academic medical centers. J Am Coll Surg. 2001;193:1–11. - PubMed
-
- 2004 National Physician Fee Schedule Relative Value File. Washington, DC: Centers for Medicare and Medicaid, Department of Health and Human Services; 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
