

doi: 10.1080/08998280.2005.11928030.
Pericardial heart disease: its morphologic features and its causes
Affiliations
- PMID: 16200146
- PMCID: PMC1200698
- DOI: 10.1080/08998280.2005.11928030
Item in Clipboard
Pericardial heart disease: its morphologic features and its causes
Proc (Bayl Univ Med Cent).
2005 Jan.
No abstract available
Figures
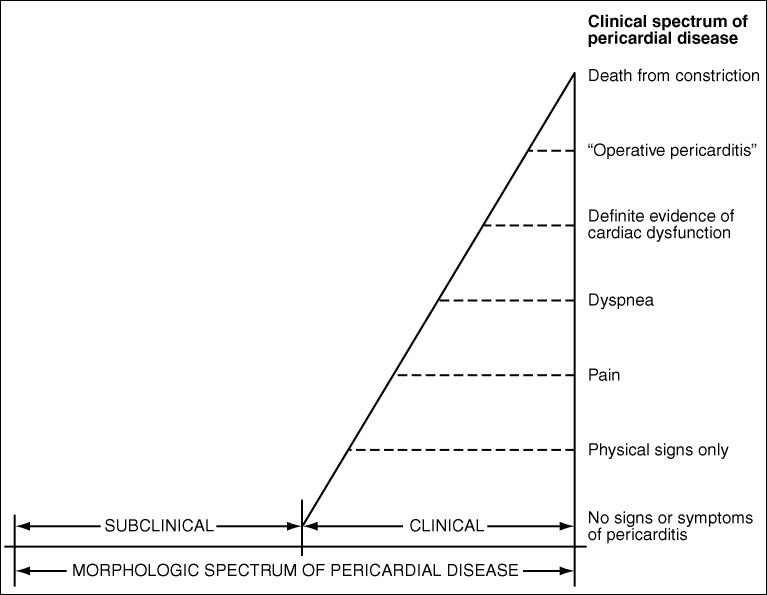
The clinical and morphologic spectrum of pericardial heart disease.
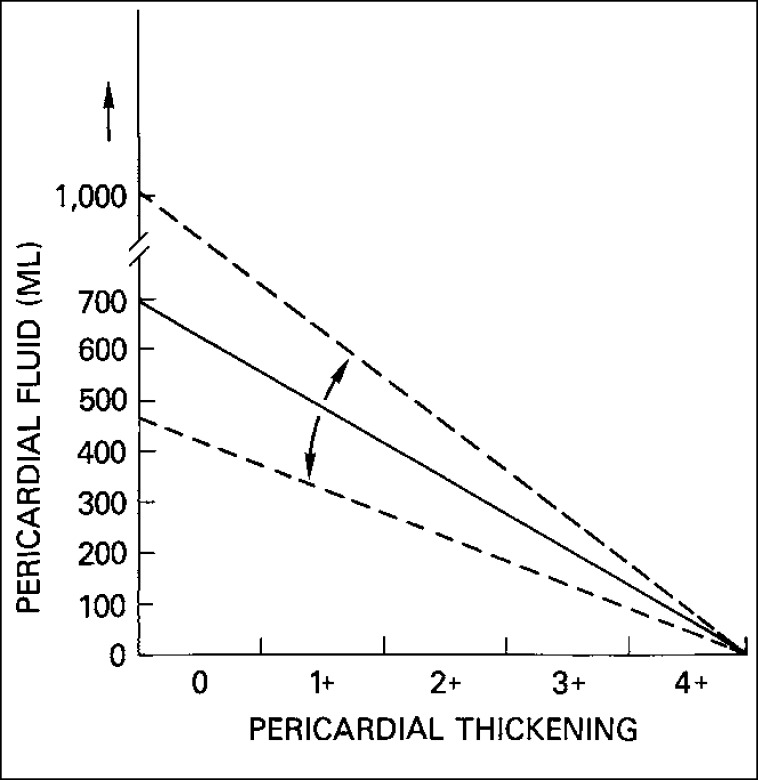
Pericardial fluid accumulation is, in general, not proportional to pericardial thickening: the more the pericardial fluid, the less the pericardial thickening and vice versa. The dashed lines on either side of the uninterrupted line indicate that the latter may be shifted by an acute or chronic course. Less fluid is needed to produce tamponade if the fluid accumulation is rapid than if it is slow. Likewise, less pericardial thickening is needed to produce constriction if the thickening occurs rapidly as opposed to slowly.
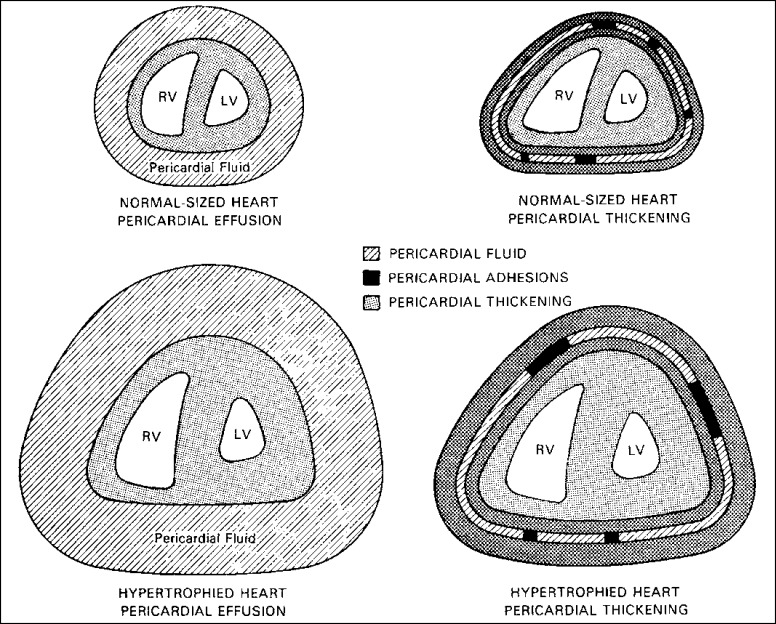
More pericardial fluid or thicker pericardia is necessary to constrict a hypertrophied heart than a normal-sized one. RV indicates right ventricle; LV, left ventricle.
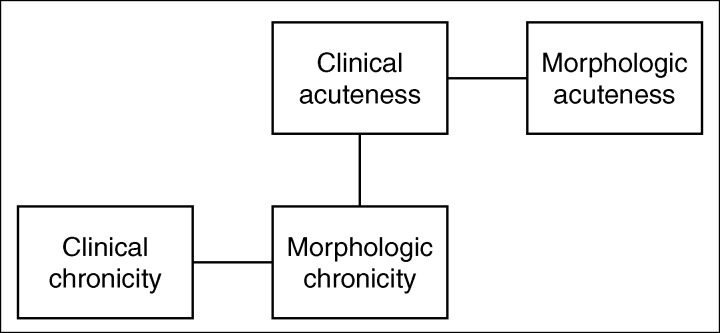
Relationship between the clinical and morphologic features in pericardial heart disease. Although clinical and morphologic acuteness and clinical and morphologic chronicity often go together, a chronic morphologic process can present acutely.
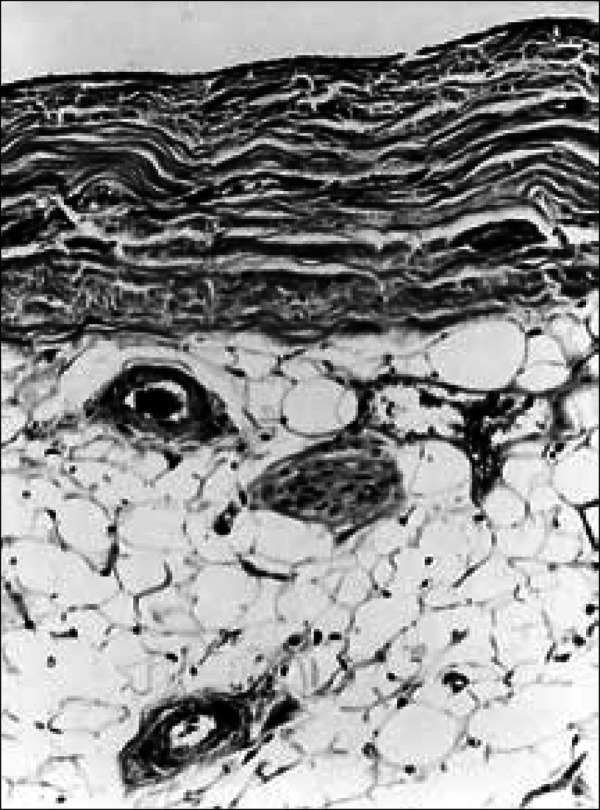
Normal parietal pericardium. A single layer of mesothelial cells covers the layer of dense fibrous tissue on the cardiac side. On the mediastinal side of the fibrous layer is adipose tissue, and in it are located vascular channels and nerves. Masson stain, ⋇185.
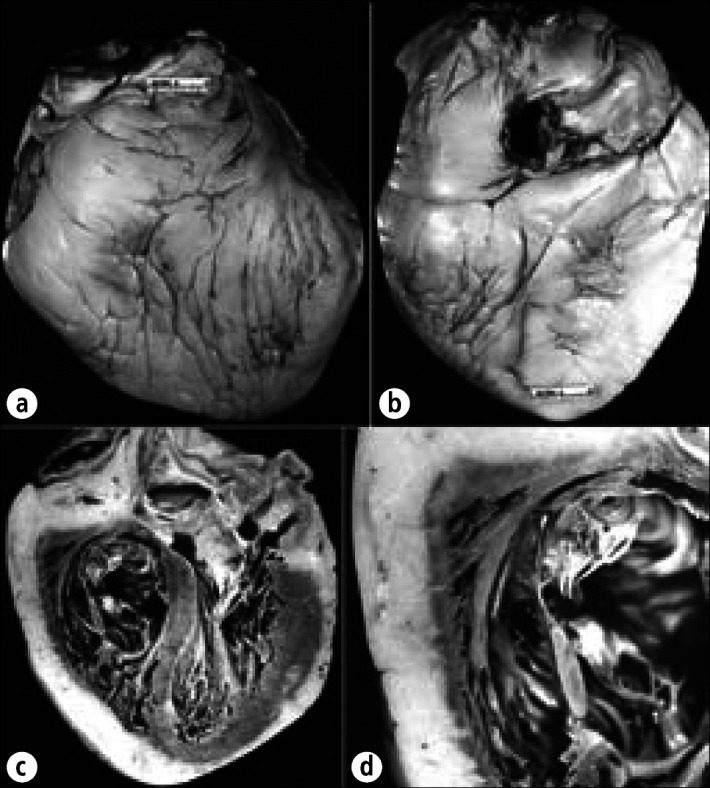
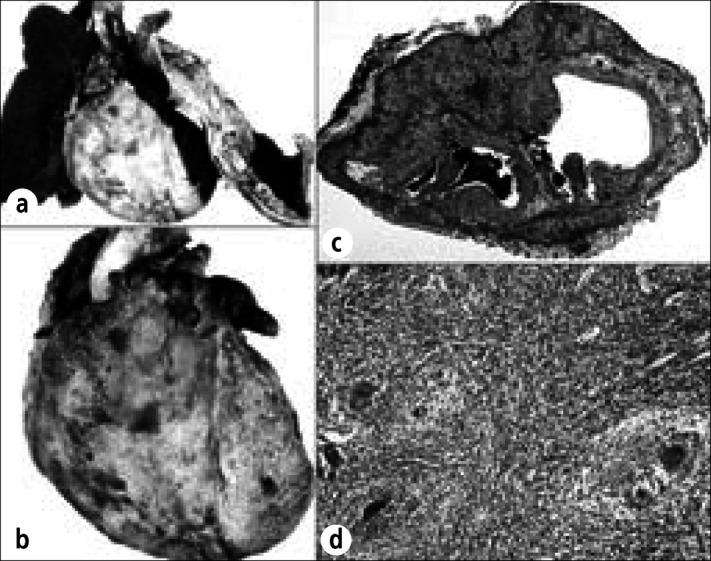
Massive increase in subepicardial adipose tissue in an 82-year-old man with idiopathic hemochromatosis. The myocardium was completely covered by fat. The heart weighed 500 gm. (a) Anterior view. (b) Posterior view. (c) Longitudinal section showing the thickness of fat compared with the thickness of the myocardial wall. (d) Close-up view of the right ventricular wall. The cause of the massive subepicardial adiposity in this patient is not certain.
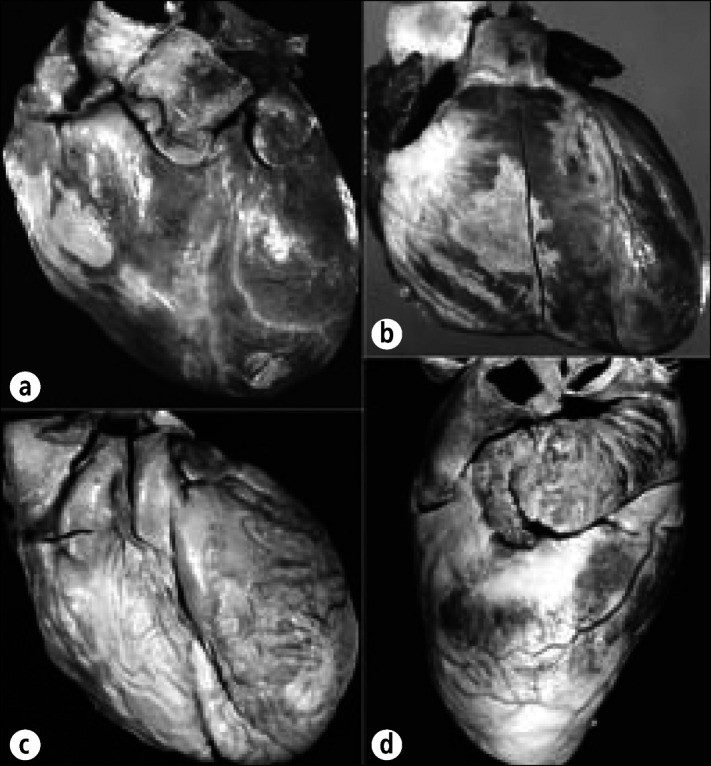
Epicardial collagen plaques (soldier's plaques, milk spots) in the hearts of 4 different patients. (a) Collagen plaques are present over the right ventricle and over the left ventricular apex. (b) A discrete collagen plaque is visible over the right ventricle. (c) Virtually the entire right ventricle and pulmonary trunk are covered by a collagen plaque. (d) The lateral view shows the collagen plaques just beneath the left atrial appendage and over the left ventricular apex. Note that the subepicardial adipose tissue is relatively sparse in the 4 patients. When more subepicardial fat is present, epicardial collagen plaques are less likely to form.
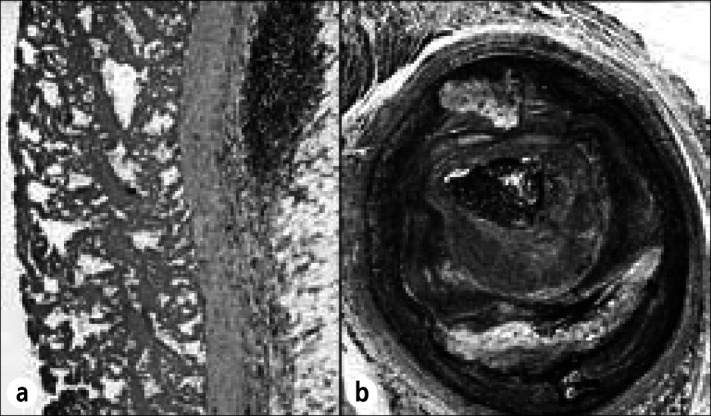
Diffuse fibrinous pericarditis from acute myocardial infarction. This 56-year-old man developed a precordial friction rub on day 6 following infarction and died on day 16. (a) A deposit of fibrin covers the mildly thickened epicardium. (b) The left circumflex coronary artery is completely occluded by both atherosclerotic plaque and thrombus. Hematoxylin-eosin stain, ⋇28 (a); Movat stain, ⋇14 (b).
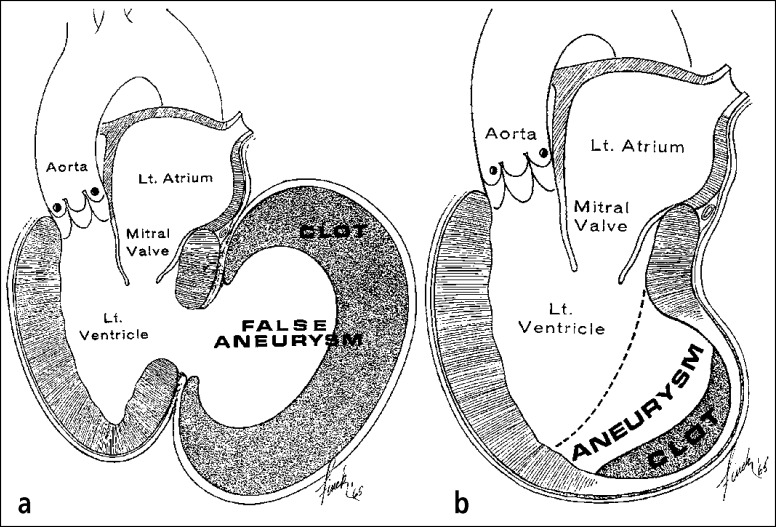
(a) False vs (b) true left ventricular aneurysms with adherent parietal pericardia. The wall of the false aneurysm is parietal pericardium, which had adhered to the epicardium before the left ventricle ruptured. In the true aneurysm, the parietal pericardium adheres to the scarred left ventricular myocardium, but the actual wall of the aneurysm had been myocardium at one time.
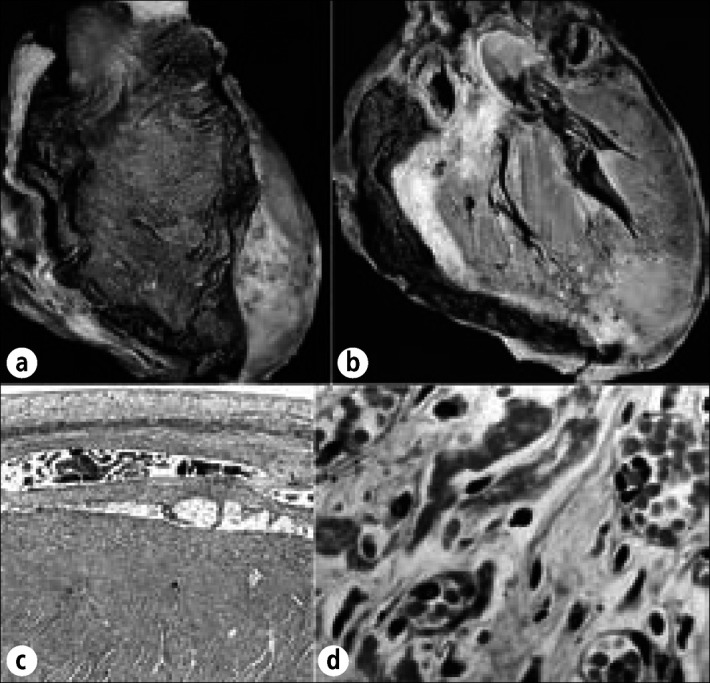
Hemorrhagic pericardial heart disease in chronic renal disease. This 26-year-old woman had renal failure and pericardial effusion on admission 3 weeks before death. Pericardiocentesis was performed twice, but cardiac tamponade progressed. At necropsy, 800 mL of hemorrhagic fluid was present and the pericardia were diffusely thickened and covered by fibrin deposits and blood clots. (a) Exterior view of the heart anteriorly. (b) Longitudinal section of the heart. The pericardial space over the left ventricle is obliterated. (c) Photomicrograph showing adherence of the parietal pericardium to underlying visceral pericardium over the left ventricle. (d) Close-up portion of the epicardium showing many vascular channels, the presumed source of the hemorrhagic pericardial effusion. Phosphotungstic acid hematoxylin, ⋇7.5 (c); hematoxylin-eosin stain; ⋇628 (d).
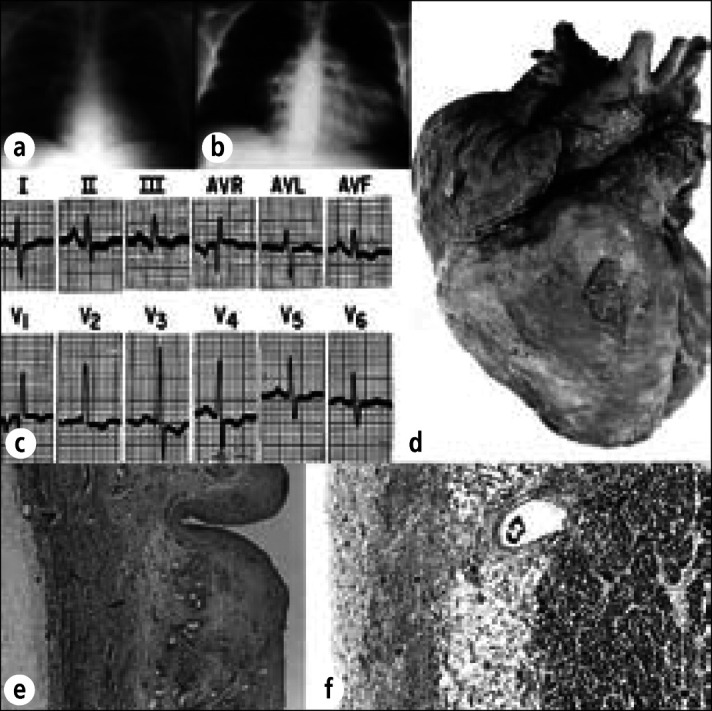
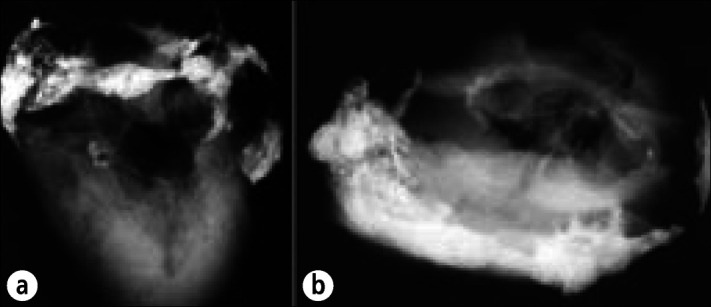
Hemorrhagic pericardial heart disease in a 30-year-old man with Gaucher's disease and pulmonary hypertension (from Gaucher cells plugging pulmonary capillaries). Chest radiographs (a) 2 months before death and (b) day of death, demonstrating marked enlargement of the cardiac silhouette. About 750 mL of blood was present in the pericardial sac. (c) Electrocardiogram recorded 1 hour before death. (d) Exterior of the heart showing diffuse fibrinous pericarditis and marked enlargement of the right atrium and ventricle. (e) Thickened parietal pericardium containing large vascular channels. (f) Thickened visceral pericardium. The cause of the hemorrhagic pericardial effusion was not determined. Periodic acid-Schiff stain, ⋇22 (e), ⋇33 (f).
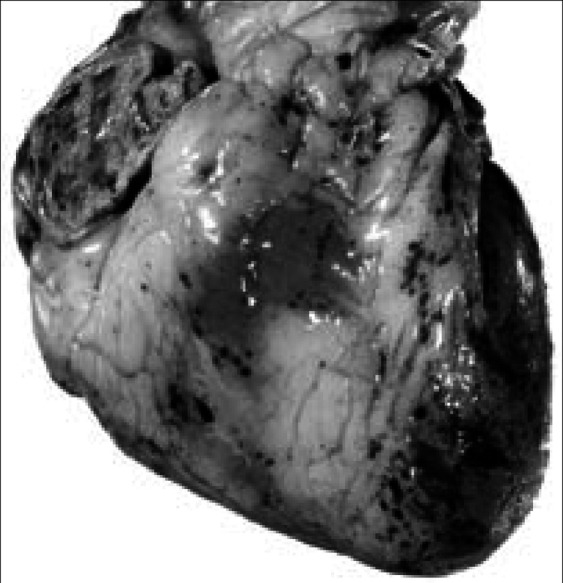
Focal epicardial hemorrhages in hypothrombocytopenia. The anterior surface of the heart shows focal hemorrhages in a 56-year-old man with acute myelogenous leukemia. The epicardial hemorrhages seen here are typical of those observed in many patients with severe hypothrombocytopenia from any cause. This man's platelet count 2 days before death was 500 per mm3.
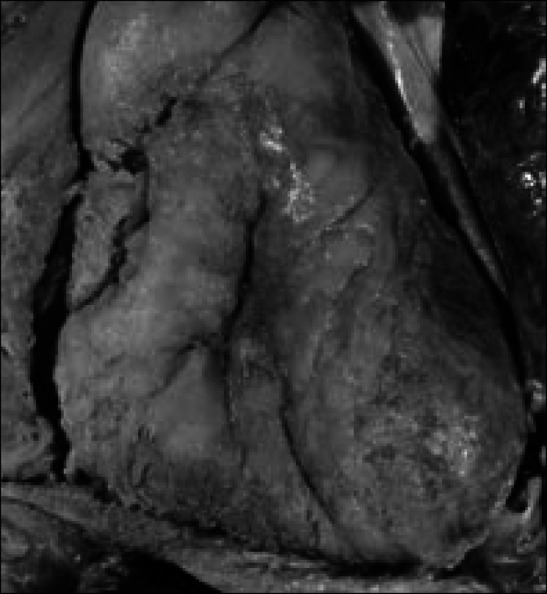
Purulent pericarditis in the exterior of the heart in a 56-year-old man with squamous cell carcinoma arising in the floor of the mouth. He developed a neoplastic abscess cavity in the left posterior mediastinum, and it opened into the esophagus, bronchus, left pleural cavity, and pericardial sac. Candida albicans was cultured from the purulent material in the pericardial sac.
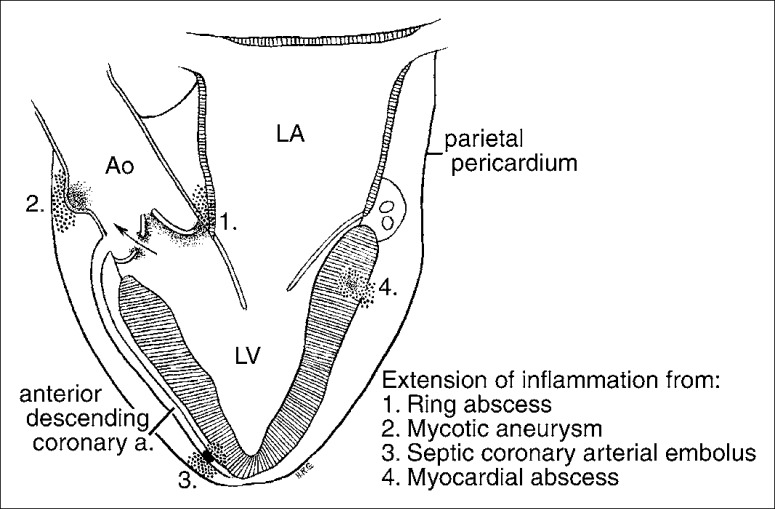
Schematic portrayal of the pathogenesis of pericarditis in infective endocarditis. Ao indicates aorta; LV, left ventricle; LA, left atrium.
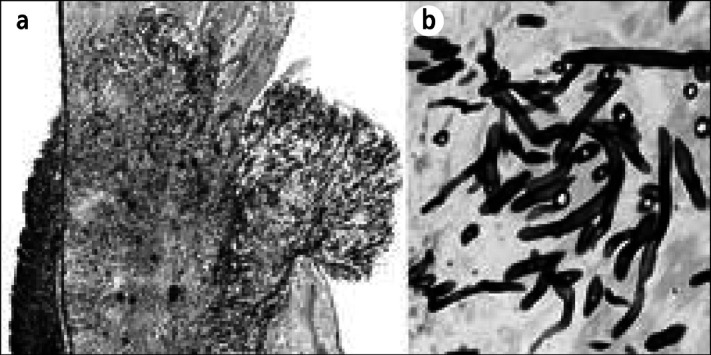
Candida tropicalis pancarditis in a 7-year-old girl with acute lymphocytic leukemia and a 21-month illness. The child never had signs or symptoms of cardiac disease but died of disseminated candidiasis. (a) Section of the right atrial wall with fungi extending from the epicardium through the myocardium into the endocardium. (b) Close-up of Candida organisms. Methenamine silver stain, ⋇12 (a), ⋇520 (b).
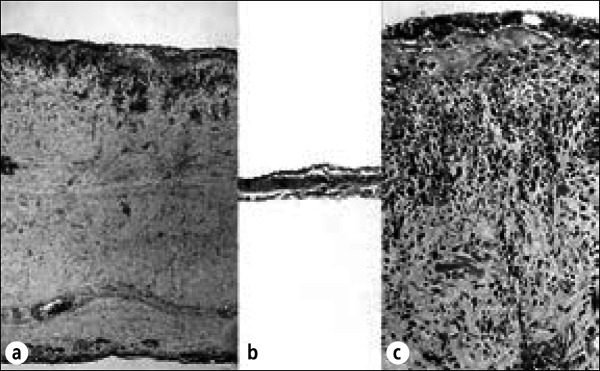
Radiation pericarditis. Stage IIIB Hodgkin's disease was diagnosed in this 54-year-old man, and he then received radiation therapy to the mediastinum. Eighteen months later, he developed recurrent pericardial effusion and signs of pericardial constriction, including elevated venous pressure and congestive cardiac failure. He underwent pericardiectomy, and at operation the pericardial sac contained about 150 mL of fluid. The parietal and visceral pericardia were focally adherent by fibrinous adhesions. After excision of the anterior portion of parietal pericardium, which was up to 1.0 cm in thickness, the central venous pressure dropped from 15 to 8 cm of water. The patient had an uneventful recovery and no further symptoms of myocardial constriction. (a) Section of parietal pericardium showing diffuse fibrous thickening with fibroblast proliferation. Plasma cells and lymphocytes are present. (b) Section of normal pericardium for comparison. (c) Higher-power view of parietal pericardium in this patient showing fibroblasts, lymphocytes, and plasma cells. These changes are characteristic of radiation pericarditis. Hematoxylin-eosin stain, ⋇27 (a and b), ⋇160 (c).
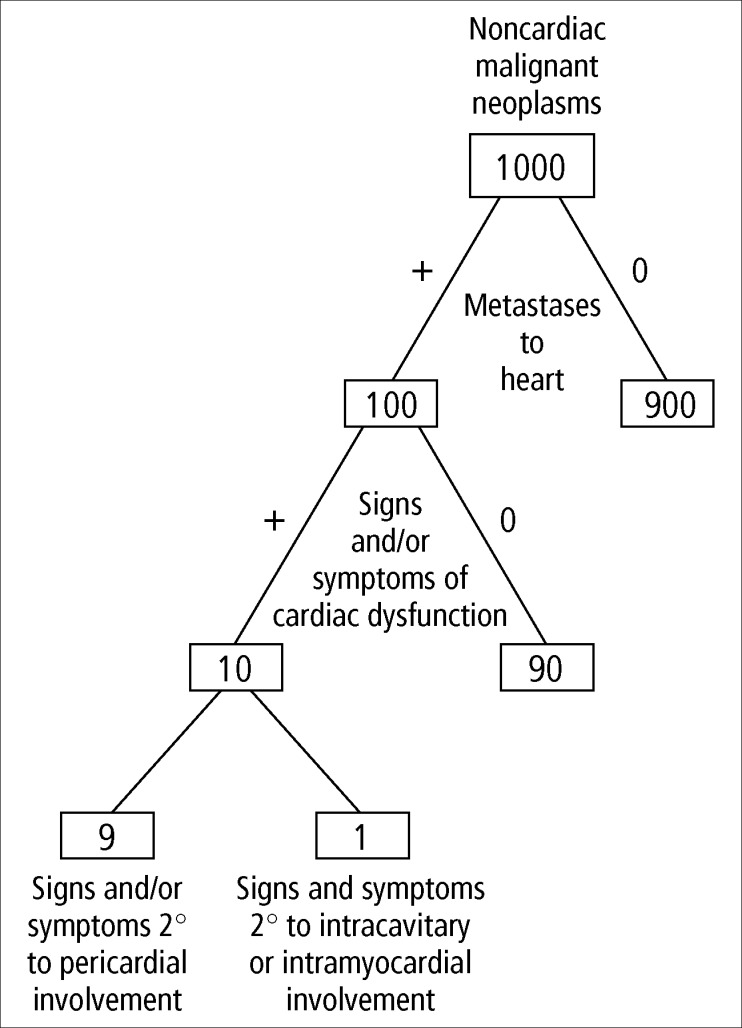
The frequency of pericardial involvement in malignant neoplasms.
Tuberculous pericarditis in a 45-year-old dyspneic man whose chest radiograph showed complete loss of volume of the left lung and massive left pleural effusion. Congestive cardiac failure and respiratory insufficiency led to death. At necropsy, the entire left lung was collapsed, and the left hemithorax was filled with pus. The left pleura was markedly thickened and focally calcified. No granulomas or foci of caseation necrosis were observed in either lung or in the hilar lymph nodes. (a) Heart and lungs showing loss of left lung, cardiomegaly (600 gm), and diffuse pericarditis. (b) Closer view of the exterior of the heart showing fibrinous exudate covering the entire myocardial surface. (c) Section of the left atrial appendage showing complete involvement of the epicardium by caseating granulomas and giant cells. Fibrinous pericardial exudate also covers most of its surface. (d) High-power view of granulomas covering the left atrial appendage. No acid-fast organisms were found. Hematoxylin-eosin stain, ⋇5 (c); periodic acid-Schiff stain, ⋇80 (d).
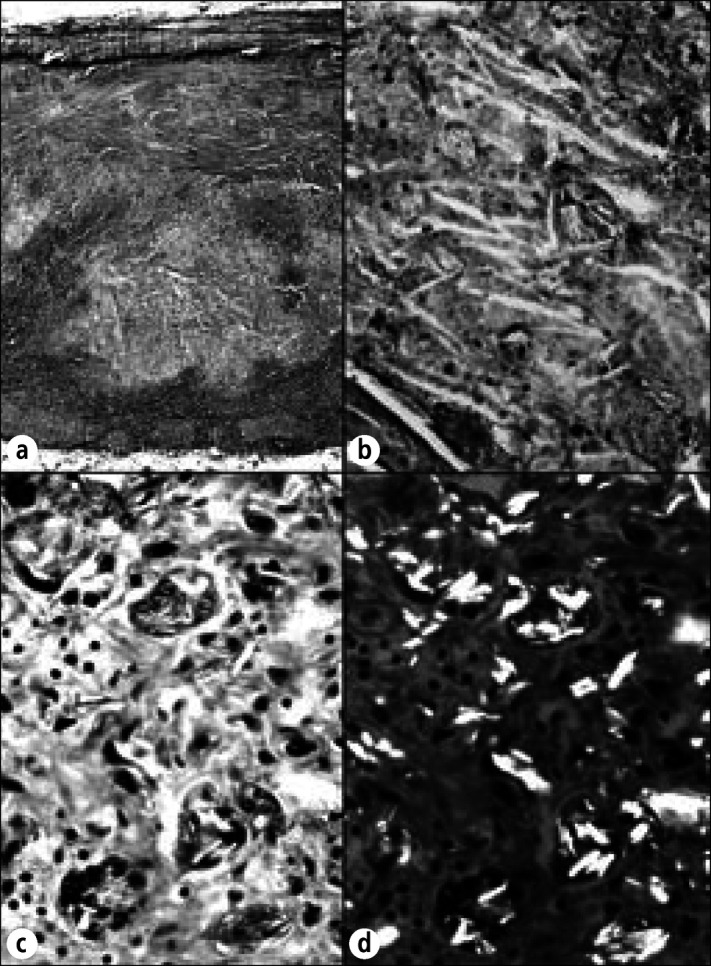
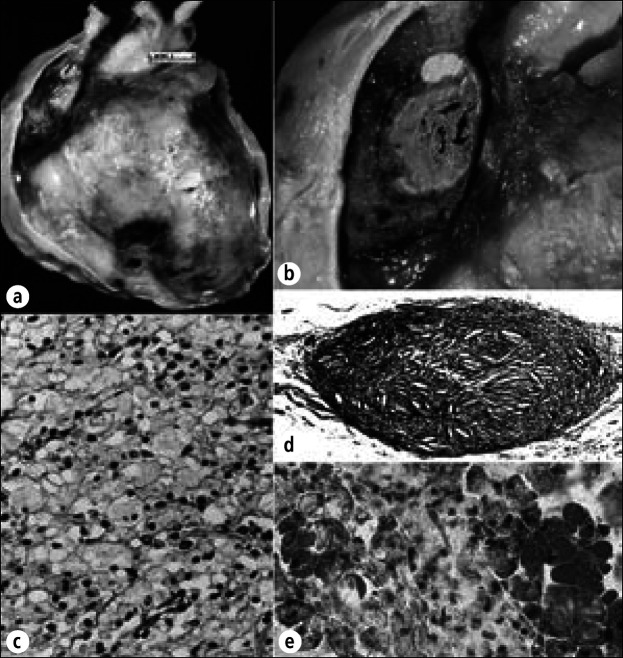
Talc-induced granulomatous pericarditis in a 92-year-old woman who was stated to have had angina pectoris beginning at age 63. At age 67, she underwent talcum-powder sprinkling on her pericardium (Beck or Thompson procedure). Immediately preoperatively, she was in congestive heart failure with atrial fibrillation and a slow ventricular response. At necropsy, an old healed anterolateral apical infarct was present, but no myocardial necrosis was observed. The striking finding, however, was a diffuse fibrous and granulomatous pericarditis secondary to talc with complete obliteration of the pericardial space. (a) Section of parietal pericardium showing large foci of acellular debris containing multiple cholesterol clefts. (b) Higher-power view showing cholesterol clefts and talc. (c) Multinucleated foreign-body giant cells with intracellular talc granules. A few mononuclear cells are present. (d) Same field as (c) with polarization showing highly refractile talc particles both intracellularly and extracellularly. Hematoxylin-eosin stain, ⋇23 (a), ⋇250 (b), ⋇480 (c, d).
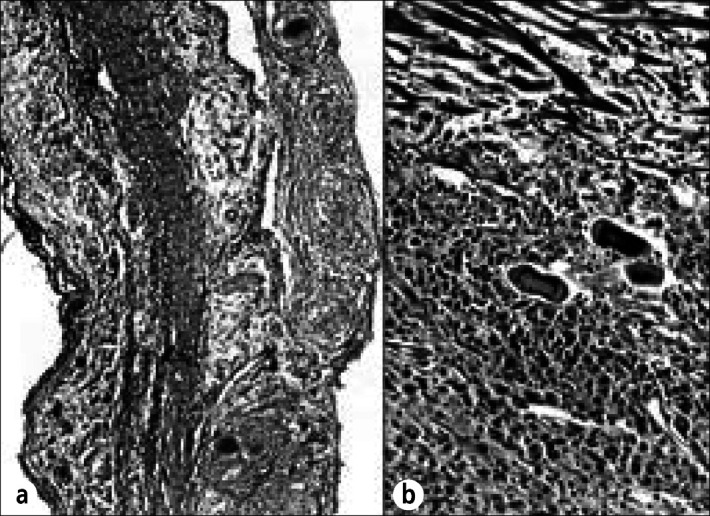
Sarcoidosis of the pericardium in a 47-year-old woman who was well until 16 months before death, when exertional dyspnea appeared. Thereafter, there was clinical evidence of recurring pleural and pericardial effusions. She died of progressive respiratory insufficiency. At necropsy, both lungs were extensively infiltrated by noncaseating granulomas devoid of microorganisms. Grossly, the pericardium and myocardium contained no focal lesions except in the left ventricular papillary muscles. On histologic examination, however, noncaseating granulomas were found in the (a) parietal pericardium and (b) visceral pericardium. In addition to the noncaseating granulomas in the papillary muscle, similar microscopic-sized granulomas were observed in the walls of all 4 cardiac chambers. Hematoxylin-eosin stain, ⋇80 (a), ⋇220 (b).
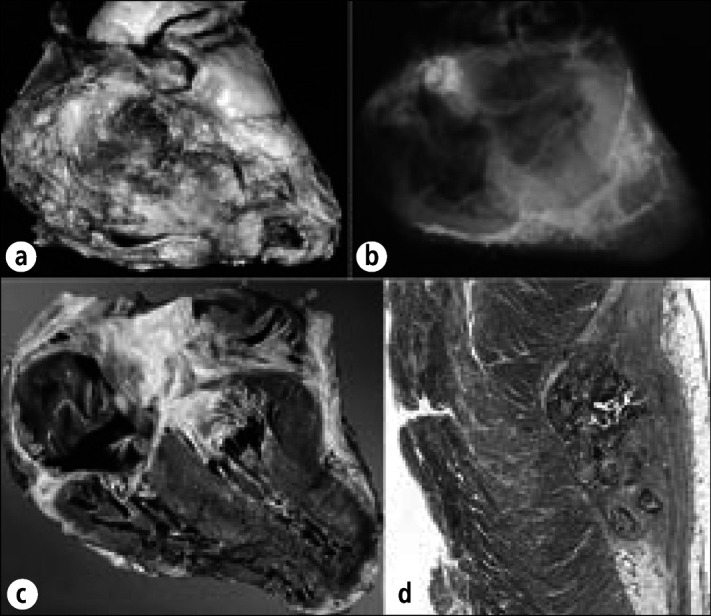
Calcific pericardial heart disease in a 78-year-old man, an alcoholic with cirrhosis, esophageal varices, and chronic pancreatitis, who died of a gastrointestinal hemorrhage. No evidence of cardiac dysfunction was ever present clinically. At necropsy the pericardial space was obliterated by fibrous adhesions. The adherence of the parietal to the visceral pericardium could not be separated over the right atrioventricular sulcus. The cardiac chambers, valves, and coronary arteries were normal. The right atrioventricular sulcus was extensively infiltrated by calcific deposits. Radiographs of the heart specimen at necropsy: (a) anteroposterior view; (b) cephalad caudal view. Calcific deposits also are present in the mitral anulus.
Calcific constrictive pericardial heart disease in a 68-year-old man who had had pericardiectomies for relief from constriction 15 and 7 years before death. Terminally, evidence of myocardial constriction reappeared. Chylous ascites secondary to obstruction of the thoracic duct by carcinoid tumor also were present. At necropsy, the heart weighed 530 gm. Diffuse obliterative constrictive pericarditis was present, and the remaining parietal pericardium was bound down to the epicardium by fibrous tissue. The inferior and superior venae cavae were enlarged, and the right atrium and pulmonary trunk were dilated. Yellow intimal streaks were seen in the pulmonary arteries, suggesting pulmonary arterial hypertension. Histologic sections showed fibrous thickening with calcific deposits of the pericardia with occasional collections of lymphocytes, plasma cells, and histiocytes, but no granulomas. The intrapulmonary arteries had thickened walls. No granulomas were found in the lungs. The cause of the pericardial constriction was never determined. (a) Exterior of the heart. (b) Radiograph of the heart showing residual calcific deposits over the ventricles. (c) Longitudinal section of the heart showing right atrial dilatation and right ventricular hypertrophy. (d) Section of left ventricle compressed by overlying calcific deposit. Hematoxylin-eosin stain, ⋇3.
Cholesterol pericardial heart disease in a 34-year-old woman with hypothyroidism. She was short and stocky and had enlarged earlobes, bilateral hypoplastic fourth toes, receding hairline, small tongue, and no menstruation. She had orthopnea, pedal edema, and hypoactive deep tendon reflexes. Chest radiograph showed a globular-shaped cardiac silhouette and clear lung fields, and angiogram showed an 18-mm-thick pericardial effusion. Despite diuresis, the pedal edema persisted. Pleuritic-type anterior chest pain appeared, and a 15-mm paradoxic pulse pressure was measured. Pericardiocentesis produced 500 mL of cloudy golden-colored fluid. The polyethylene catheter was left in place and over the next 5 days, 2 L of fluid was removed. Fluid cholesterol was 165 mg/dL; serum cholesterol was 355 mg/dL. The patient improved after pericardiocentesis but became anuric following aortography and died. (a) Exterior surface of the heart and pericardium showing thickening of the parietal pericardium and focal deposits of cholesterol (yellow) over the right ventricle. (b) View of thickened parietal pericardium over the right atrial appendage and an epicardial cholesterol deposit. (c) Foam cells in the cholesterol deposit shown in (b). (d) Cholesterol granuloma in the pericardium showing cholesterol clefts and a foreign body reaction. (e) Frozen section of epicardial deposits stained for lipid. The foam cells stain strongly for lipid. Hematoxylin-eosin stain, ⋇400 (c), ⋇50 (d); oil-red O stain, ⋇400 (e).
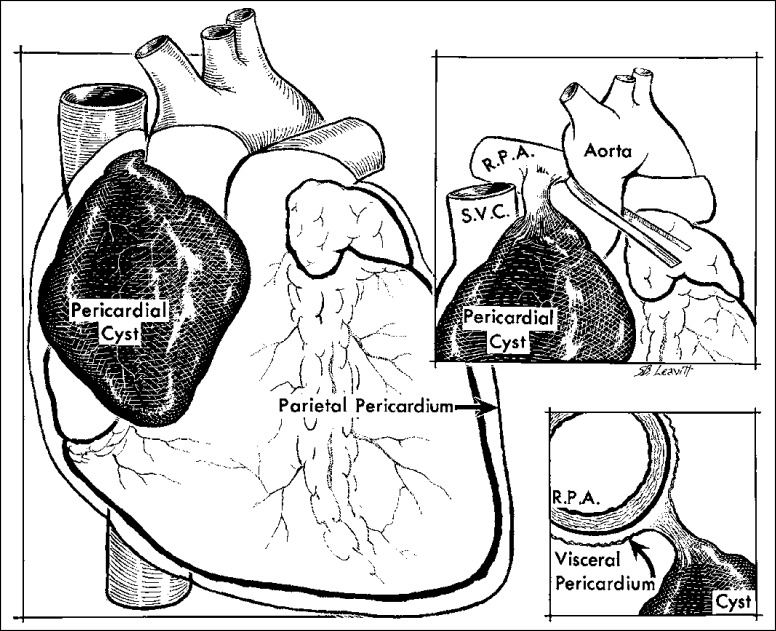
Pericardial cyst, an incidental necropsy finding in a 75-year-old woman. The cyst, which contained serous fluid, overlay the right atrium and arose from a pedicle attached to the right main pulmonary artery (RPA). SVC indicates superior vena cava.
Similar articles
-
Pericardial heart disease: a study of its causes, consequences, and morphologic features.Cardiovasc Clin. 1976;7(3):11-65. Cardiovasc Clin. 1976. PMID: 1000531
-
Pericardial heart disease.Curr Probl Cardiol. 1977 Jun;2(3):1-71. doi: 10.1016/0146-2806(77)90006-8. Curr Probl Cardiol. 1977. PMID: 142612 Review.
-
Morphologic aspects of pericardial heart disease: Part I.Clin Cardiol. 1992 Mar;15(3):203-9. doi: 10.1002/clc.4960150312. Clin Cardiol. 1992. PMID: 1551268
-
Morphologic aspects of pericardial heart disease: Part II.Clin Cardiol. 1992 Apr;15(4):291-8. doi: 10.1002/clc.4960150413. Clin Cardiol. 1992. PMID: 1563133 Review.
-
Pericardial fluid from patients with ischemic heart disease induces myocardial cell apoptotis via an oxidant stress-sensitive p38 mitogen-activated protein kinase pathway.J Mol Cell Cardiol. 2001 Mar;33(3):419-30. doi: 10.1006/jmcc.2000.1314. J Mol Cell Cardiol. 2001. PMID: 11181011
Cited by
-
Spontaneous cardiac calcinosis in BALB/cByJ mice.Comp Med. 2013 Feb;63(1):29-37. Comp Med. 2013. PMID: 23561935 Free PMC article.
-
"Bread and butter" fibrinous pericarditis.Autops Case Rep. 2016 Dec 30;6(4):5-7. doi: 10.4322/acr.2016.050. eCollection 2016 Oct-Dec. Autops Case Rep. 2016. PMID: 28210567 Free PMC article. No abstract available.
-
Cardiac mesothelial papillary hyperplasia in four dogs.J Vet Diagn Invest. 2018 May;30(3):479-482. doi: 10.1177/1040638717753964. Epub 2018 Jan 11. J Vet Diagn Invest. 2018. PMID: 29322883 Free PMC article.
-
Cancer Treatment-Associated Pericardial Disease: Epidemiology, Clinical Presentation, Diagnosis, and Management.Curr Cardiol Rep. 2019 Nov 25;21(12):156. doi: 10.1007/s11886-019-1225-6. Curr Cardiol Rep. 2019. PMID: 31768769 Review.
-
External Compression of Epicardial Coronary Arteries with Partial Calcific Pericarditis.Heart Views. 2017 Jan-Mar;18(1):26-29. doi: 10.4103/1995-705X.206207. Heart Views. 2017. PMID: 28584590 Free PMC article.
References
-
- Osler W. Designed for the Use of Practitioners and Students of Medicine. New York: Appleton Co; 1892. The Principles and Practice of Medicine; p. 1079.
-
- Reeves RL. Cause of acute pericarditis. Am J Med Sci. 1953;225:34. - PubMed
-
- Griffith GC, Wallace L. The etiology of pericarditis. Am Heart J. 1949;37:636.
-
- Ishihara T, Ferrans VJ, Jones M, Boyce SW, Kawanami O, Roberts WC. Histologic and ultrastructural features of normal parietal pericardium. Am J Cardiol. 1980;46:744–753. - PubMed
-
- Shirani J, Berezowski K, Roberts WC. Quantitative measurement of normal and excessive (cor adiposum) subepicardial adipose tissue, its clinical significance, and its effect on electrocardiographic QRS voltage. Am J Cardiol. 1995;76:414–418. - PubMed
LinkOut - more resources
Full Text Sources