

Lack of interchangeability between visual analogue and verbal rating pain scales: a cross sectional description of pain etiology groups
- PMID: 16202149
- PMCID: PMC1274324
- DOI: 10.1186/1471-2288-5-31
Lack of interchangeability between visual analogue and verbal rating pain scales: a cross sectional description of pain etiology groups
Abstract
Background: Rating scales like the visual analogue scale, VAS, and the verbal rating scale, VRS, are often used for pain assessments both in clinical work and in research, despite the lack of a gold standard. Interchangeability of recorded pain intensity captured in the two scales has been discussed earlier, but not in conjunction with taking the influence of pain etiology into consideration.
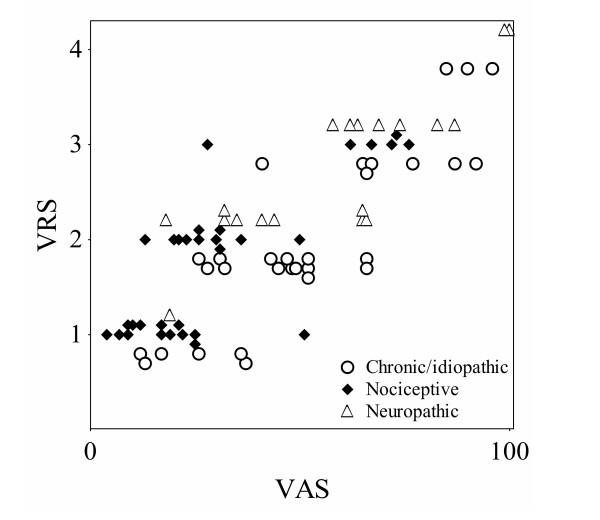
Methods: In this cross-sectional study, patients with their pain classified according to its etiology (chronic/idiopathic, nociceptive and neuropathic pain) were consecutively recruited for self-assessment of their actual pain intensity using a continuous VAS, 0-100, and a discrete five-category VRS. The data were analyzed with a non-parametric statistical method, suitable for comparison of scales with different numbers of response alternatives.
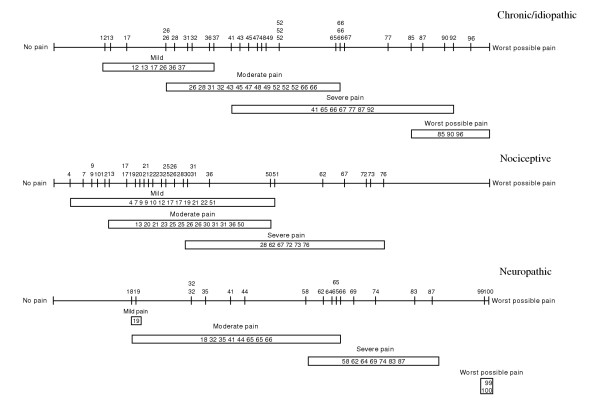
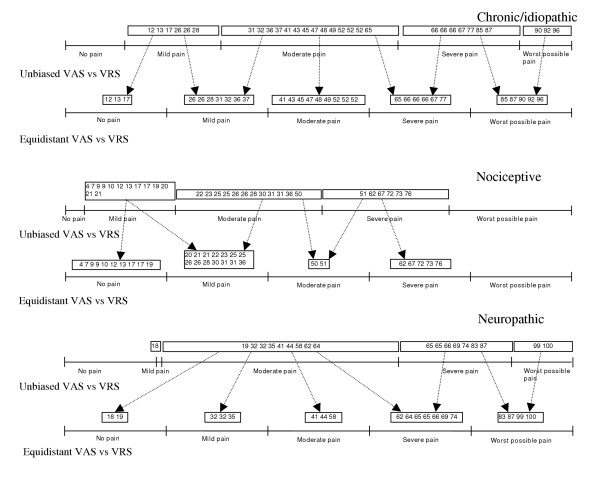
Results: An overlapping of the VAS records relative the VRS categories was seen in all pain groups. Cut-off positions for the VAS records related to the VRS categories were found lower in patients with nociceptive pain relative patients suffering from chronic/idiopathic and neuropathic pain. When comparing the VAS records transformed into an equidistant five-category scale with the VRS records, systematic disagreements between the scales was shown in all groups. Furthermore, in the test-retest a low percentage of the patients agreed to the same pain level on the VAS while the opposite hold for the VRS.
Conclusion: The pain intensity assessments on VAS and VRS are in this study, not interchangeable due to overlap of pain records between the two scales, systematic disagreements when comparing the two scales and a low percentage intra-scale agreement. Furthermore, the lower VAS cut-off positions relative the VRS labels indicate different meaning of the rated pain intensity depending on pain etiology. It is also indicated that the scales have non-linear properties and that the two scales probably have different interpretation. Our findings are in favor of using the VRS in pain intensity assessments but if still the VAS is preferred, the VAS data should be analyzed as continuous using statistical methods suitable for ordinal data. Furthermore, our findings indicate a risk to over or under estimate the patient's perceived pain when interpreting condensed VAS data.
Figures

Similar articles
-
Pain measurement: Visual Analogue Scale (VAS) and Verbal Rating Scale (VRS) in clinical trials with OTC analgesics in headache.Cephalalgia. 2012 Feb;32(3):185-97. doi: 10.1177/03331024111430856. Cephalalgia. 2012. PMID: 22332207 Clinical Trial.
-
Measuring the Intensity of Chronic Pain: Are the Visual Analogue Scale and the Verbal Rating Scale Interchangeable?Pain Pract. 2015 Jul;15(6):538-47. doi: 10.1111/papr.12216. Epub 2014 Apr 16. Pain Pract. 2015. PMID: 24735056
-
Learning from pain scales: patient perspective.J Rheumatol. 2003 Jul;30(7):1584-8. J Rheumatol. 2003. PMID: 12858463
-
Pain Intensity Assessment Scales for Dermatologic Surgery Patients: A Systematic Review.Dermatol Surg. 2022 Feb 1;48(2):232-238. doi: 10.1097/DSS.0000000000003353. Dermatol Surg. 2022. PMID: 34923536
-
Pain: a review of three commonly used pain rating scales.J Clin Nurs. 2005 Aug;14(7):798-804. doi: 10.1111/j.1365-2702.2005.01121.x. J Clin Nurs. 2005. PMID: 16000093 Review.
Cited by
-
Trajectory analysis for postoperative pain using electronic health records: A nonparametric method with robust linear regression and K-medians cluster analysis.Health Informatics J. 2020 Jun;26(2):1404-1418. doi: 10.1177/1460458219881339. Epub 2019 Oct 17. Health Informatics J. 2020. PMID: 31621460 Free PMC article.
-
Comparison of numerical and verbal rating scales to measure pain exacerbations in patients with chronic cancer pain.Health Qual Life Outcomes. 2010 Apr 22;8:42. doi: 10.1186/1477-7525-8-42. Health Qual Life Outcomes. 2010. PMID: 20412579 Free PMC article.
-
Evaluating postherniorrhaphy groin pain: Visual Analogue or Verbal Rating Scale?Hernia. 2008 Apr;12(2):147-51. doi: 10.1007/s10029-007-0301-9. Epub 2007 Nov 15. Hernia. 2008. PMID: 18004502
-
Response scale selection in adult pain measures: results from a literature review.J Patient Rep Outcomes. 2018 Sep 6;2:40. doi: 10.1186/s41687-018-0053-6. eCollection 2017. J Patient Rep Outcomes. 2018. PMID: 30238085 Free PMC article. Review.
-
The Plasticity of Brain Gray Matter and White Matter following Lower Limb Amputation.Neural Plast. 2015;2015:823185. doi: 10.1155/2015/823185. Epub 2015 Oct 25. Neural Plast. 2015. PMID: 26587289 Free PMC article.
References
-
- Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, Kerns RD, Stucki G, Allen RR, Bellamy N, Carr DB, Chandler J, Cowan P, Dionne R, Galer BS, Hertz S, Jadad AR, Kramer LD, Manning DC, Martin S, McCormick CG, McDermott MP, McGrath P, Quessy S, Rappaport BA, Robbins W, Robinson JP, Rothman M, Royal MA, Simon L, Stauffer JW, Stein W, Tollett J, Wernicke J, Witter J. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113:9–19. doi: 10.1016/j.pain.2004.09.012. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
