

Local hyperemia to heating is impaired in secondary Raynaud's phenomenon
- PMID: 16207327
- PMCID: PMC1257434
- DOI: 10.1186/ar1785
Local hyperemia to heating is impaired in secondary Raynaud's phenomenon
Abstract
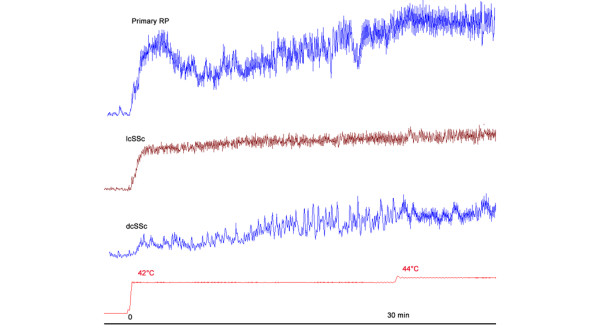
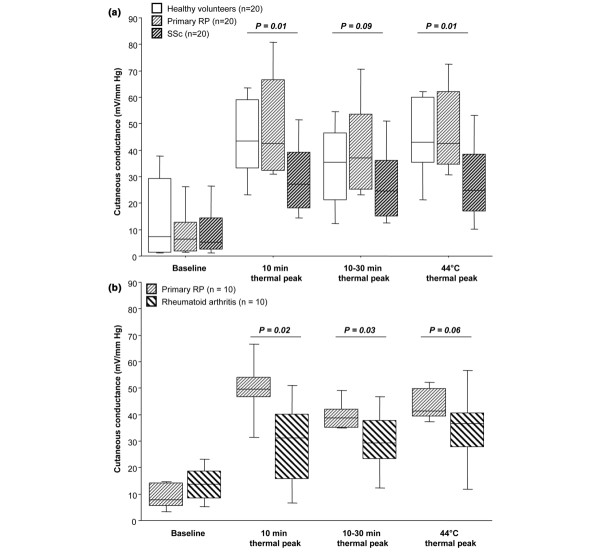
Accurate and sensitive measurement techniques are a key issue in the quantification of the microvascular and endothelial dysfunction in systemic sclerosis (SSc). Thermal hyperemia comprises two separate mechanisms: an initial peak that is axon reflex mediated; and a sustained plateau phase that is nitric oxide dependent. The main objective of our study was to test whether thermal hyperemia in patients with SSc differed from that in patients with primary Raynaud's phenomenon (RP) and healthy controls. In a first study, we enrolled 20 patients suffering from SSc, 20 patients with primary RP and 20 healthy volunteers. All subjects were in a fasting state. Post-occlusive hyperemia, 0.4 mg sublingual nitroglycerin challenge and thermal hyperemia were performed using laser Doppler flowmetry on the distal pad of the third left finger. In a second study, thermal hyperemia was performed in 10 patients with rheumatoid arthritis and 10 patients with primary RP. The thermal hyperemia was dramatically altered in terms of amplitude and kinetics in patients with SSc. Whereas 19 healthy volunteers and 18 patients with primary RP exhibited the classic response, including an initial peak within the first 10 minutes followed by a nadir and a second peak, this occurred only in four of the SSc patients (p < 0.0001). The 10 minutes thermal peak was 43.4 (23.2 to 63), 42.6 (31 to 80.7) and 27 (14.7 to 51.4) mV/mm Hg in the healthy volunteers, primary RP and SSc groups, respectively (p = 0.01), while the 44 degrees C thermal peak was 43.1 (21.3 to 62.1), 42.6 (31.6 to 74.3) and 25.4 (15 to 52.4) mV/mm Hg, respectively (p = 0.01). Thermal hyperemia was more sensitive and specific than post-occlusive hyperhemia for differentiating SSc from primary RP. In patients with rheumatoid arthritis, thermal hyperemia was also altered in terms of amplitude. Thermal hyperemia is dramatically altered in patients with secondary RP in comparison with subjects with primary RP. Further studies are required to determine the mechanisms of this altered response, and whether it may provide additional information in a clinical setting.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
