

Two-year evaluation of Borrelia burgdorferi culture and supplemental tests for definitive diagnosis of Lyme disease
- PMID: 16207966
- PMCID: PMC1248466
- DOI: 10.1128/JCM.43.10.5080-5084.2005
Two-year evaluation of Borrelia burgdorferi culture and supplemental tests for definitive diagnosis of Lyme disease
Erratum in
- J Clin Microbiol. 2007 Jan;45(1):277
Abstract
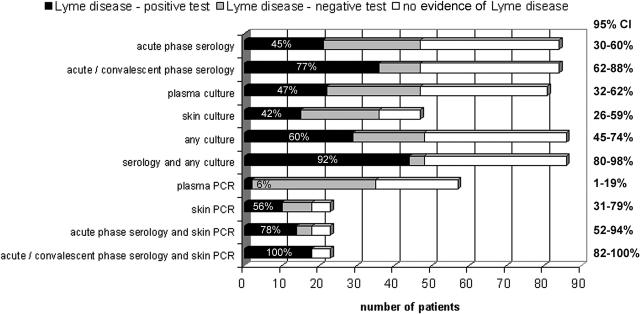
Lyme disease is usually diagnosed and treated based on clinical manifestations. However, laboratory testing is useful for patients with confusing presentations and for validation of disease in clinical studies. Although cultivation of Borrelia burgdorferi is definitive, prior investigations have shown that no single test is optimal for Lyme disease diagnosis. We applied high-volume blood culture, skin biopsy culture, PCR, and serodiagnosis to a cohort of patients with suspected Lyme disease acquired in Maryland and southern Pennsylvania. The study was performed to confirm the relative utility of culture and to identify laboratory testing algorithms that will supplement clinical diagnosis. Overall, 30 of 86 patients (35%) were culture positive, whereas an additional 15 of 84 (18%) were seropositive only (51% total sero- and culture positive), and PCR on skin biopsy identified 4 additional patients who were neither culture nor seropositive. Among 49 laboratory test-positive patients, the highest sensitivity (100%) for diagnosis was obtained when culture, skin PCR, and serologic tests were used, although serologic testing with skin PCR was almost as sensitive (92%). Plasma PCR was infrequently positive and provided no additional diagnostic value. Although culture is definitive and has a relatively high sensitivity, the results required a mean of 3.5 weeks to recovery. The combination of acute-phase serology and skin PCR was 75% sensitive, offering a practical and relatively rapid alternative for confirming clinical impression. The full battery of tests could be useful for patients with confusing clinical signs or for providing strong laboratory support for clinical studies of Lyme disease.
Figures
Comment in
-
Evaluation of tests for Lyme disease.J Clin Microbiol. 2006 Apr;44(4):1616; author reply 1616-7. doi: 10.1128/JCM.44.4.1616-1617.2006. J Clin Microbiol. 2006. PMID: 16597916 Free PMC article. No abstract available.
References
-
- Auwaerter, P. G., J. Aucott, and J. S. Dumler. 2004. Lyme borreliosis (Lyme disease): molecular and cellular pathobiology and prospects for prevention, diagnosis and treatment. Expert Rev. Mol. Med. 2004:1-22. - PubMed
-
- Centers for Disease Control and Prevention. 1995. Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. Morb. Mortal. Wkly. Rep. 44:590-591. - PubMed
-
- Centers for Disease Control and Prevention. 1997. Case definitions for infectious conditions under public health surveillance. Morb. Mortal. Wkly. Rep. 46(RR10):1-55. - PubMed
-
- Centers for Disease Control and Prevention. 2004. Lyme disease—United States, 2001-2002. Morb. Mortal. Wkly. Rep. 53:365-368. - PubMed
-
- Dumler, J. S. 2001. Molecular diagnosis of Lyme disease: review and meta-analysis. Mol. Diagn. 6:1-11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
