

Family aggregation of upper airway soft tissue structures in normal subjects and patients with sleep apnea
- PMID: 16210668
- PMCID: PMC2662941
- DOI: 10.1164/rccm.200412-1736OC
Family aggregation of upper airway soft tissue structures in normal subjects and patients with sleep apnea
Abstract
Rationale: Sleep apnea is believed to be a genetic disorder. Thus, we hypothesized that anatomic risk factors for sleep apnea would demonstrate family aggregation.
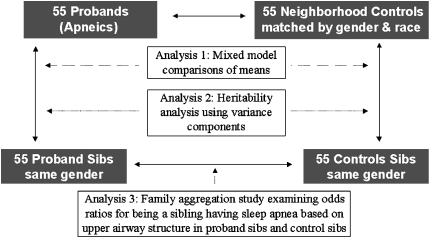
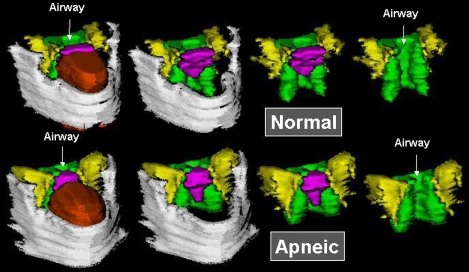
Objectives: We used volumetric magnetic resonance imaging in a sib pair "quad" design to study the family aggregation of the size of upper airway soft tissue structures that are associated with increased risk for obstructive sleep apnea.
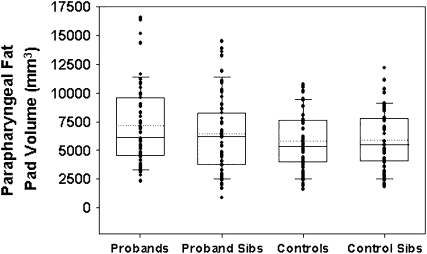
Methods: We examined 55 sleep apnea probands (apnea-hypopnea index [AHI]: 43.2 +/- 26.3 events/h), 55 proband siblings (AHI: 11.8 +/- 16.6 events/h), 55 control subjects (AHI: 2.1 +/- 1.7 events/h), and 55 control siblings (AHI: 4.2 +/- 4.0 events/h). The study design used exact matching on ethnicity and sex, frequency matching on age, and statistical control for visceral neck fat and craniofacial dimensions.
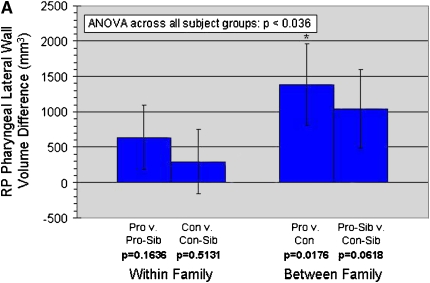
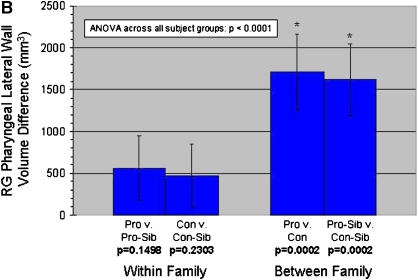
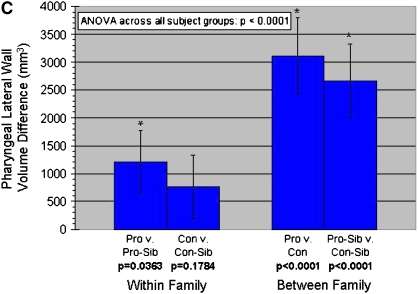
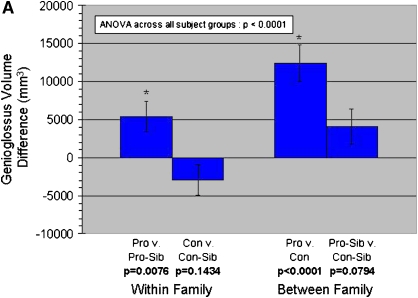
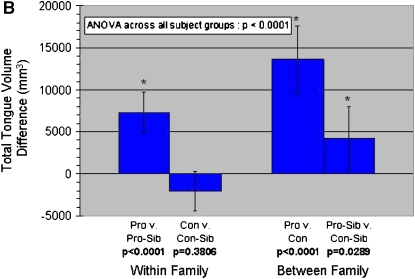
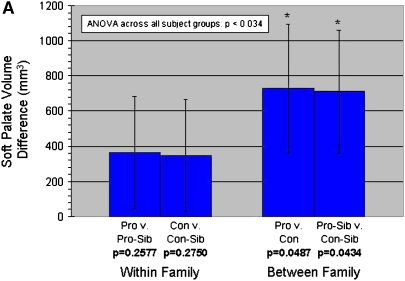
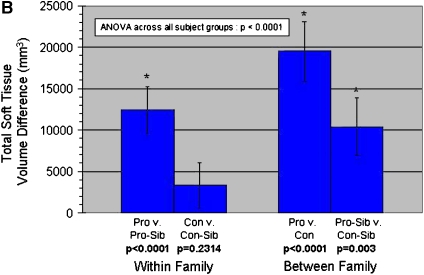
Measurements and main results: The data support our a priori hypothesis that the volume of the important upper airway soft tissue structures is heritable. The volume of the lateral pharyngeal walls (h(2) = 36.8%; p = 0.001), tongue (h(2) = 36.5%; p = 0.0001), and total soft tissue (h(2) = 37.5%; p = 0.0001) demonstrated significant levels of heritability after adjusting for sex, ethnicity, age, visceral neck fat, and craniofacial dimensions. In addition, our data indicate that heritability of the upper airway soft tissue structures is found in normal subjects and patients with apnea. Thus, it is not simply a consequence of the prevalence of apnea.
Conclusions: This is the first time family aggregation of size of the upper airway soft tissue structures has been demonstrated.
Figures
References
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 2002;165:1217–1239. - PubMed
-
- Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, D'Agostino RB, Newman AB, Lebowitz MD, Pickering TG. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community- based study. JAMA 2000;283:1829–1836. - PubMed
-
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–1384. - PubMed
-
- Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, O'Connor GT, Boland LL, Schwartz JE, Samet JM. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 2001;163:19–25. - PubMed
-
- Palmer LJ, Redline S. Genomic approaches to understanding obstructive sleep apnea. Respir Physiolo Neurobiol 2003;135:187–205. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical