

Comparison of functional MR imaging guidance to electrical cortical mapping for targeting selective motor cortex areas in neuropathic pain: a study based on intraoperative stereotactic navigation
- PMID: 16219831
- PMCID: PMC7976154
Comparison of functional MR imaging guidance to electrical cortical mapping for targeting selective motor cortex areas in neuropathic pain: a study based on intraoperative stereotactic navigation
Abstract
Purpose: To assess the concordance between data from functional MR imaging (fMRI) guidance and the intraoperative electrical cortical mapping (iCM) in targeting selective motor cortex areas in refractory neuropathic pain.
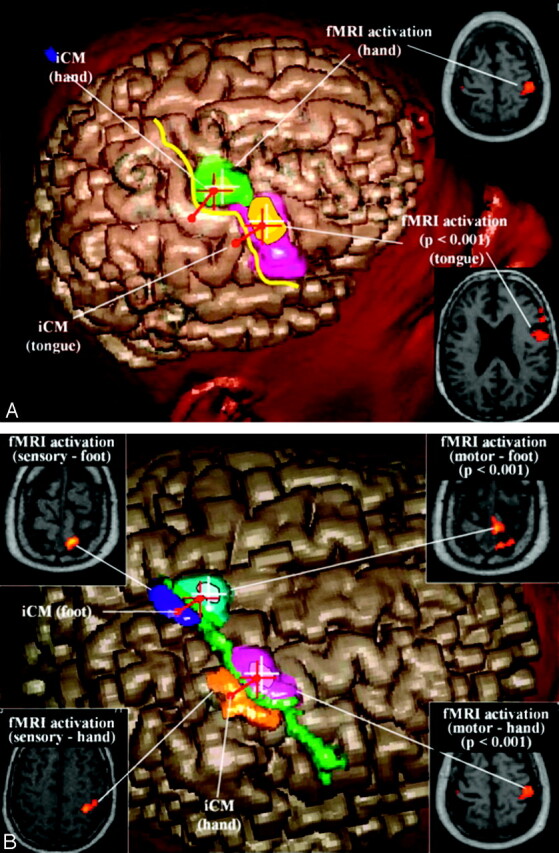
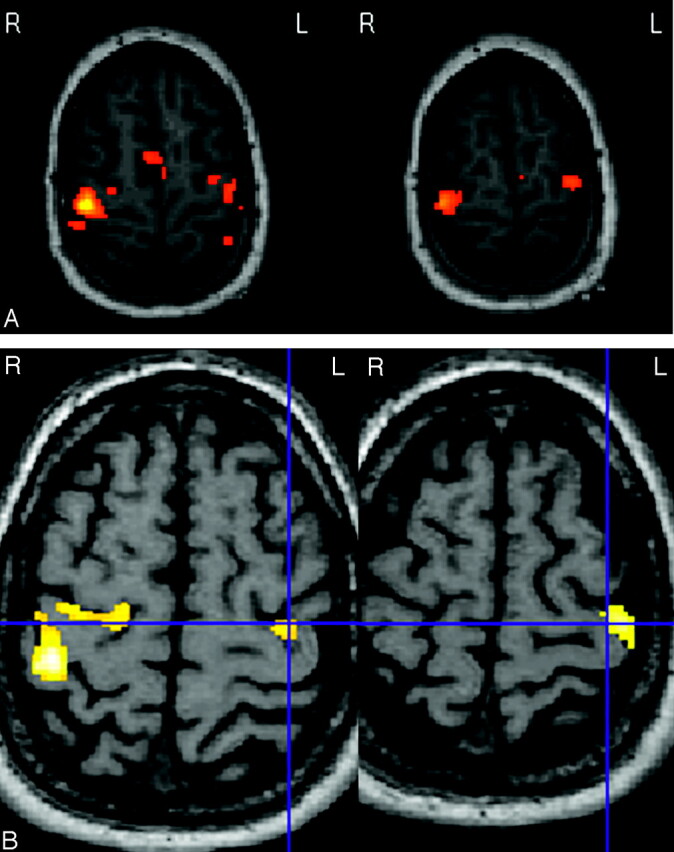
Methods: Twenty-one patients (11 women and 10 men; mean age, 55.6 years) with refractory central (ischemic, 8 cases) and neuropathic pain (trigeminal neuropathy, 6 cases; syrinx/amputation/plexus trauma, 7 cases) underwent surgery for the implantation of an epidural electrode for chronic motor cortex stimulation (MCS) with general anesthesia and a frameless neuronavigation system used for the image-guided targeting procedure. All patients were studied by preoperative fMRI and epidural iCM with somatosensory evoked potentials and motor cortex stimulodetection. fMRI investigated systematically motor tasks of both hands and that related to the somatic area (foot or tongue) affected by pain. fMRI data were analyzed with the Statistical Parametric Mapping99 software (initial analysis threshold [AT] corresponding to P < .001), registered in the neuronavigation system and correlated intraoperatively with iCM. Matching of fMRI and iCM was specifically examined, focusing the study on hand mapping.
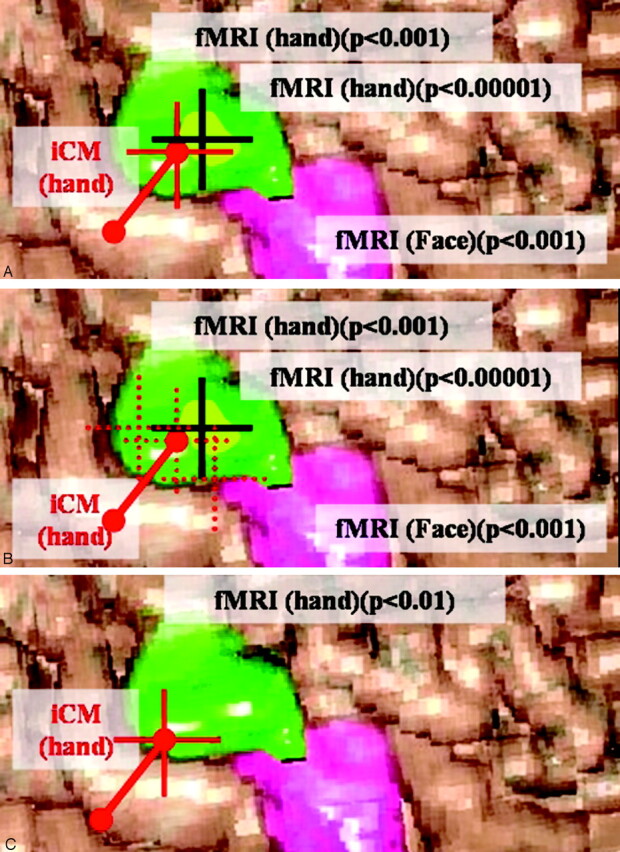
Results: Concordance between contours of fMRI activation area and iCM in precentral gyrus (mean distance, 3.8 mm) was found in 20/21 patients (95%). Because precision of iCM was suboptimal in 7 patients, concordance for more restrictive values of the AT (P < .0001) was found in only 13 of these 20 patients. Concordance was not found in one patient, as result of image distortion and residual motion artifact.
Conclusions: In this study, fMRI guidance provides information that matches those of an independent functional method. These data illustrate the functional accuracy of fMRI guidance for the operative targeting of selective motor cortex areas in neuropathic pain.
Figures
Similar articles
-
Combination of functional magnetic resonance imaging-guided neuronavigation and intraoperative cortical brain mapping improves targeting of motor cortex stimulation in neuropathic pain.Neurosurgery. 2005 Apr;56(2 Suppl):344-59; discussion 344-59. doi: 10.1227/01.neu.0000144837.31665.29. Neurosurgery. 2005. PMID: 15794831
-
Combination of functional magnetic resonance imaging-guided neuronavigation and intraoperative cortical brain mapping improves targeting of motor cortex stimulation in neuropathic pain.Neurosurgery. 2008 Jun;62(6 Suppl 3):941-56. doi: 10.1227/01.neu.0000333762.38500.ac. Neurosurgery. 2008. PMID: 18695580
-
The Zeiss-MKM system for frameless image-guided approach in epidural motor cortex stimulation for central neuropathic pain.Neurosurg Focus. 2001 Sep 15;11(3):E3. doi: 10.3171/foc.2001.11.3.4. Neurosurg Focus. 2001. PMID: 16519423 Clinical Trial.
-
Motor cortex stimulation for neuropathic pain.Acta Neurochir Suppl. 2007;97(Pt 2):37-44. doi: 10.1007/978-3-211-33081-4_4. Acta Neurochir Suppl. 2007. PMID: 17691287 Review.
-
Extradural cortical stimulation for central pain.Acta Neurochir Suppl. 2007;97(Pt 2):27-36. doi: 10.1007/978-3-211-33081-4_3. Acta Neurochir Suppl. 2007. PMID: 17691286 Review.
Cited by
-
Cortical mapping and frameless stereotactic navigation in the high-field intraoperative magnetic resonance imaging suite.J Neurosurg. 2009 Dec;111(6):1185-90. doi: 10.3171/2009.5.JNS09164. J Neurosurg. 2009. PMID: 19499978 Free PMC article.
-
Motor cortex stimulation for facial chronic neuropathic pain: A review of the literature.Surg Neurol Int. 2012;3(Suppl 4):S290-311. doi: 10.4103/2152-7806.103023. Epub 2012 Oct 31. Surg Neurol Int. 2012. PMID: 23230534 Free PMC article.
-
Invasive brain stimulation for the treatment of neuropathic pain.Nat Rev Neurol. 2011 Sep 20;7(12):699-709. doi: 10.1038/nrneurol.2011.138. Nat Rev Neurol. 2011. PMID: 21931348 Review.
-
Comparison of navigated transcranial magnetic stimulation and functional magnetic resonance imaging for preoperative mapping in rolandic tumor surgery.Neurosurg Rev. 2013 Jan;36(1):65-75; discussion 75-6. doi: 10.1007/s10143-012-0413-2. Epub 2012 Aug 11. Neurosurg Rev. 2013. PMID: 22886323
-
Neuroimaging and neuromodulation: complementary approaches for identifying the neuronal correlates of tinnitus.Front Syst Neurosci. 2012 Apr 9;6:15. doi: 10.3389/fnsys.2012.00015. eCollection 2012. Front Syst Neurosci. 2012. PMID: 22509155 Free PMC article.
References
-
- Braun V, Dempf S, Tomczak R, et al. Functional cranial neuronavigation: direct integration of fMRI and PET data. J Neuroradiol 2000;27:157–163 - PubMed
-
- Braun V, Dempf S, Tomczak R, et al. Multimodal cranial neuronavigation: direct integration of functional magnetic resonance imaging and positron emission tomography data: technical note. Neurosurgery 2001;48:1178–1181 - PubMed
-
- Cosgrove GR, Buchbinder BR, Jiang H. Functional magnetic resonance imaging for intracranial navigation. Neurosurg Clin N Am 1996;7:313–322 - PubMed
-
- Heilbrun MP. Optimization of cranial resections. Stereotact Funct Neurosurg 2001;76:140–144 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical